In this article 
View /
Download pdf version of this article
Whaia te iti kahurangi – Ki te tuohu koe, me he maunga teitei, ko Aoraki anake
Pursue excellence – should you stumble, let it be to a lofty mountain
Key Concepts
- In New Zealand, acute rheumatic fever is now almost exclusively a disease affecting Māori and Pacific peoples
- People who have had acute rheumatic fever require secondary prophylaxis for at least ten years to reduce the risk
of developing chronic rheumatic heart disease
- Cases of acute rheumatic fever, rheumatic heart disease and the number of deaths due to chronic rheumatic heart disease
are increasing in New Zealand
- Primary care clinicians need to know the risk of rheumatic fever in their community and to encourage at-risk people
to seek a consultation when they have a sore throat
- In high-risk areas, all Māori and Pacific children who present with a sore throat should have a throat swab
taken and antibiotics prescribed empirically if any red flags are present
Things are getting worse, not better...
The rate of Acute Rheumatic Fever (ARF) in New Zealand is increasing. Between 2005 and 2010, the rate of ARF doubled
from 1.9 reported cases per 100 000 population to 3.8 per 100 000 (Figure 1).1 The majority of cases are occurring
in low socioeconomic communities in the northern and central North Island and in pockets around the Wellington region.
ARF is 23 times more likely in Māori and nearly 50 times more likely in Pacific peoples than in other ethnic groups.2 From
1996 to 2005, while ARF rates significantly decreased amongst New Zealand Europeans, rates amongst Māori and Pacific
children increased significantly. Although comprising just 4.7% of the New Zealand population, this group represented
almost 60% of all cases reported.3 It is widely believed that this over representation is due to a combination
of overcrowded living conditions, poverty and decreased access to treatment options.
Other than New Zealand, and indigenous populations in Australia and the Pacific Islands, ARF is a disease of the developing
world. What primary health care services in New Zealand can do is to:
- Understand there is a problem
- Be aware of the New Zealand guidelines and algorithms for the management of ARF
- Assist in raising community awareness, and support early detection programmes in high-risk areas
- Continue to lobby for improvements and equality in socioeconomic factors
What is acute rheumatic fever?
Acute rheumatic fever is an autoimmune response to a group A streptococcus (GAS) infection, usually in the upper respiratory
tract. The resulting transitory, generalised, inflammatory response may affect the heart, joints, central nervous system
and skin. The chief concern is the inflammation of the heart (carditis), as this may cause cardiac valve stenosis. ARF
has no known genetic basis and occurs mainly in children aged five to 14 years, peaking around age eight. ARF is rare
in children aged under three years, as the immune system has not developed sufficiently to allow an autoimmune response
to occur.4
In New Zealand, ARF has been a notifiable disease since 1986. Despite this, it is likely that there are significantly
more cases of ARF in New Zealand than are currently being reported to health services. A 2008 review of ARF cases (1999–2007)
in the Bay of Plenty and Lakes Districts DHBs found 147 cases, where only 75 had been previously reported.5 Factors
identified as contributing to under reporting by health professionals included; difficulty of ARF diagnosis, multiple
health professionals being involved at multiple institutions and health professionals being unfamiliar with reporting
requirements due to a lack of experience with ARF or as a result of being trained overseas. It is also likely that some
patients will not present unless the symptoms are severe.
Rheumatic heart disease is a long-term consequence of acute rheumatic fever
Over 60% of people with ARF will have long-term heart damage, termed chronic rheumatic heart disease (RHD), if left
untreated.8 RHD can cause complications later in life, particularly in a person’s 30s and 40s. Approximately
145 people in New Zealand die each year from RHD.9–11
People who have RHD have a higher risk of developing infective endocarditis and need to maintain good oral hygiene and
attend regular dental check-ups. Dentists and other health professionals need to know if a patient has RHD, as it increases
the risk of infection. Patients who have been identified as being at risk are given wallet cards (see Appendix H of Heart
Foundation guidelines4) to present to health professionals. These cards contain recommended doses of additional
antibiotics that may be required for various procedures, e.g. dental procedures involving bleeding of gingival tissues.
Sore throats mean different things in different places
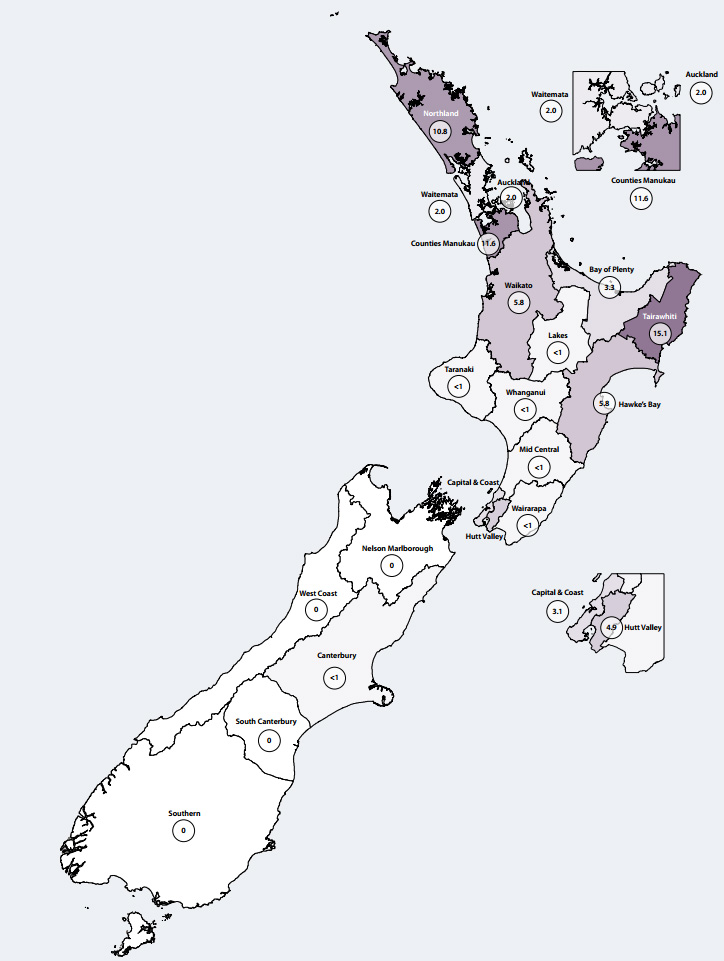
Rates of ARF vary throughout New Zealand. It is important that primary care clinicians know the approximate rate of
ARF in their communities (Figure 2).
Practices in northern and central North Island and Porirua should be on high-alert for ARF and the group A streptococcus
(GAS) throat infections that cause it. Māori and Pacific peoples have higher rates of GAS infections than New Zealand
Europeans.6 However, awareness at a national level is required given the high degree of mobility amongst the
young adult population.
Overcrowding, economic deprivation and decreased treatment opportunities also increase the risk of a person developing
ARF.7 When a patient presents with a sore throat, assessing these factors during consultation indicates the
risk that person may have of developing ARF.
Figure 2: Annual rate of rheumatic fever first admissions by DHB in New Zealand (2010)
per 100 000 population1
Think differently about sore throats
Most sore throats are viral in origin, but approximately 10% of sore throats in adults and 15–30% of sore throats in
children are due to GAS infections.5 GAS is droplet spread with a cross-infection rate of 19–50% within a household.12
Treatment of GAS sore throats with penicillin V (phenoxymethylpenicillin) or amoxicillin is considered the first-line
treatment for preventing ARF.13 Note that this is an update to the National Heart Foundation sore
throat guidelines, which recommend penicillin V as first-line treatment and amoxicillin as second-line.14 Amoxicillin
is more palatable and may be taken with food, which may encourage increased compliance with treatment, compared to pencillin
V.
Antibiotics, as outlined in Table 1, should be prescribed to patients for the first or second instance of GAS sore throat
in a three month period. Other recommendations are provided for recurrent cases of GAS infection (see sore throat algorithm,
Heart Foundation guidelines).14
Table 1: Recommended treatment for GAS positive sore throats (Algorithm 4 - Guide for sore throat management,
National Heart Foundation, 2006, Lennon D et al, 2011)13,14
The following information has been updated, please see
http://www.ttophs.govt.nz/vdb/document/1056 for the latest information.
| Antibiotic |
Route |
Regimen |
Duration |
| First choice |
| Penicillin V |
Oral (on empty stomach) |
Children: 20 mg/kg per day in two to three divided doses. Maximum 500 mg, three times daily
Adults: 500 mg, twice daily |
10 days |
| Amoxicillin |
Oral |
Weight <30 kg: 750 mg, once daily
Weight >30 ;kg: 1500 mg, once daily |
10 days |
| Alternatives |
| Erythromycin ethyl succinate (EES) if documented allergy to penicillin |
Oral |
Children: 40 mg/kg/day in two to four divided doses, to a maximum of 1 g/day
Adults: 400 mg, twice daily |
10 days |
| Benzathine penicillin G (BPG) if compliance with 10 day regimen an issue |
IM |
Weight <20 kg: 600 000 U once
Weight >20 kg: 1 200 000 U once |
Single dose |
Some General Practitioners may be reluctant to prescribe antibiotics empirically due to messages about the “Wise
Use of Antibiotics”, which have reduced antibiotic use and patient’s expectations for receiving them for colds
and sore throats during winter months. It is important that practices understand that wise use means carefully selecting
patients who might benefit from antibiotics, rather than avoiding prescribing completely. In most cases, ARF can be prevented
if antibiotics are taken within nine days of onset of symptoms.
Throat swabs
Culture of a throat swab is the best way to confirm a GAS infection. Running a standard, sterile microbiological swab
over the tonsils, back of the throat and any area with exudate, while avoiding the tongue and teeth, ensures a good sample
is collected. When possible the sample should be sent for culture within two hours, however a delay of up to twenty four
hours is acceptable.
Red flags for a potential GAS throat infection are:
- Temperature > 38 degrees celsius
- No cough or coryza (which may suggest a viral cause)
- Swollen anterior cervical lymph nodes
- Tonsillar swelling or exudate
In high-risk areas, all Māori and Pacific people aged between three and 45 years, who present with a sore throat,
should have a throat swab taken. Prescribe antibiotics empirically if a sore throat and any red flags are present. If
patients later return a positive GAS culture, then prescribe antibiotics if they are not already taking them.
Swabbing and treatment of entire households should occur if more than three cases of GAS sore throat occur in the same
home within a three month period. The New Zealand algorithm for sore throat management also provides guidance for managing
households and whānau in high-risk areas.
 A New Zealand algorithm for the management of sore throats is available
from the Heart Foundation website (listed at end of article).
A New Zealand algorithm for the management of sore throats is available
from the Heart Foundation website (listed at end of article).
There is more that can be done in high-risk areas
- Raising community awareness is an important tool in combating GAS infections
- When people from high-risk groups present with sore throats, validate their attendance as this helps to reinforce
good behaviour patterns
- Repeat the message – “sore throats matter” – to parents, Kaumātua, teachers, community pharmacists,
Kohanga Reo, and other influential community members
- Put up posters in practices – the National Heart Foundation website has resources available in Māori, Samoan
and Tongan languages
New Zealand guidelines recommend raising community awareness and implementing early detection and treatment of GAS sore
throats when annualised ARF rates exceed 20 per 100 000. If possible, school-based sore throat programmes should be implemented
by Public Health Units when rates exceed 50 per 100 000.12
 Best Practice tip: To find out the incidence of ARF in a specific area,
contact the Medical Officer of Health at your local Public Health Unit.
Best Practice tip: To find out the incidence of ARF in a specific area,
contact the Medical Officer of Health at your local Public Health Unit.
Diagnosing acute rheumatic fever
There is currently no diagnostic test for ARF so clinical judgement is important. New Zealand guidelines for the diagnosis
of ARF are based on the Jones criteria and are available from the Heart Foundation website (listed at
end of article).
The presence of two major symptoms, or one major and two minor symptoms, in both cases with a prior GAS infection, are
required to diagnose ARF.
Major symptoms include:
- Arthritis, the most common symptom, occurs in 75% of first attacks, usually in the larger joints such as the knees
and ankles6
- Carditis almost always affects the mitral and aortic valves and on presentation, a murmur may be heard.6 In
New Zealand, subclinical carditis confirmed by echocardiography is also considered a major symptom.
- Chorea (uncoordinated movements), often in adolescent females, especially affecting the hands, feet, tongue and face
which disappear during sleep and may only affect one side of the body. Chorea may occur following a prolonged latency
after streptococcus infection and generally resolves within six weeks.
- Erythema marginatum – rare (pink rings on the trunk and limbs)
- Subcutaneous nodules – rare, but highly specific to ARF
Minor symptoms include:
- Fever which accompanies most cases of ARF, except when chorea is present
- Joint pain
- Elevated CRP >30 mg/L or ESR >50 mm/h
- A prolonged P-R interval on ECG
Antistreptolysin O titre is used to confirm the diagnosis, as less than 10% of people with ARF have GAS positive throat
swabs. Assuming no re-infection, antibody levels return to normal in six to 12 months.
All patients with suspected ARF should be referred to hospital for confirmation of the diagnosis. Hospitalisation also
provides an opportunity to educate whānau about the condition and the importance of preventing recurrent attacks.
Rheumatic fever registers
Rheumatic fever registers are an important tool for managing patient compliance to secondary prophylaxis, particularly
when people move. Registers are also necessary for analysing epidemiology and channelling financial resources into regions
with the greatest need. The Auckland rheumatic fever register was established in 1981 to streamline antibiotic delivery
to patients. The subsequent clinic-based prophylaxis programme saw recurrent rheumatic fever attacks fall from 20% of
total hospital admissions for rheumatic fever to 6%.18 Further, widespread reductions would be likely if a
national rheumatic fever register was established.
Recurrent acute rheumatic fever
Recurrent rheumatic fever occurs when people who have previously had ARF are re-infected with GAS. Recurrent attacks
greatly increase the chance of a person developing RHD. Secondary prophylaxis reduces the incidence of recurrent ARF.
However, it is of major concern that the mortality rate in New Zealand due to RHD is increasing.10,15
Māori and Pacific people have the highest recurrence rates of rheumatic fever. In Auckland, between the 1980s and
1999, recurrence rates dropped from 22% to 5.5%, but in 1999, all reported recurrent cases of rheumatic fever occurred
in Māori or Pacific peoples.16 In 2008, 10% of all cases of ARF in the Bay of Plenty and Lakes District
DHBs were recurrences.
After contracting ARF, prevention of recurrent rheumatic fever requires intra-muscular injections of benzathine penicillin
G (BPG) every four weeks for a minimum of ten years. This has been shown to be safe and effective when delivered by community
nursing staff in schools, workplaces or homes.17 Secondary prophylaxis also reduces the impact of RHD, and
has been shown to be associated with a reduction in heart disease of 50–70% and decreased mortality.4
When intramuscular injections are not possible, oral penicillin V (250 mg, twice daily) can be prescribed. In cases
of penicillin sensitivity, oral erythromycin (children 40 mg/kg/day in two to four divided doses, adolescents and adults
400 mg, twice daily) is the treatment recommended by the National Heart Foundation.4
Patients receiving prophylactic treatment should only stop receiving BPG injections following specialist consultation.
Eradication of rheumatic fever
On 26 April 2011, a group of 40 health professionals from areas of high prevalence for rheumatic fever met to discuss
a pathway to achieve eradication of the disease. The National Steering Group and the Ministry of Health are now working
closely to achieve this goal.
Presentations from Professor Diana Lennon, Dr Pat Tuohy and representatives from high risk areas outlined the cross-sectoral
approach to managing rheumatic fever, including what has worked and what has not. Workshop groups then discussed health
promotion, the role of primary care, monitoring progress and integration with other childhood illness.
An over-arching theme was the need to bring all initiatives and knowledge together to ensure cohesion, quality processes
and success.
Key recommendations from the workshops included:
- Community based and whānau centred approaches with appropriate consultation are required for successful health
promotion and community awareness
- Nurse management of sore throat is an effective means of assuring accessible and affordable care in high risk areas.
Flaxmere, Kaikohe and Porirua provide current best practice examples. A “walk in” basis is important with
no financial barriers, with training supported by PHOs as part of existing continuing medical education (CME).
- Ensure parents know that prescriptions for children aged under six years are free of charge (or for those with a
prescription subsidy card, Community Services card or High User Health card).
- Increase awareness of the importance of completing the ten day antibiotic course. Amoxicillin once daily is a good
option for increasing compliance (compared to penicillin V which needs to be given two to three times daily on an empty
stomach).
- For standardised care, IT support should be available in all practices with prompts for sore throat management. Local
adaptation and simplification of guidelines in high risk areas such as Porirua can work well.
- Sore throat management should be audited as part of continuous quality improvement in primary care in high risk areas
- Nurses and other health workers could be used to broaden access to throat swabbing in high prevalence areas (in schools
and other community settings), with appropriate linkage back into primary care for management
| Contributed by Professor Norman Sharpe, Medical
Director of the National Heart Foundation of New Zealand and acting Chair of the National Steering Group. |
Following the seminar, the current management algorithms from the Heart Foundation guidelines are being reviewed and
an agreed evidence-based approach to school and community clinics developed. The recent budget allocation of $12 million
to assist eradication highlights the importance of rheumatic fever as a now recognised marker of child health. Minister
Tariana Turia’s championing and support for this successful bid and for raising the profile of rheumatic fever
should be acknowledged. The current convergence of interest around this challenging issue allows guarded optimism that
eradication can indeed be achieved. A follow-up seminar is planned for the end of the year.
Community success stories
There is significant evidence that community driven detection and treatment strategies do reduce ARF. A 2009 meta-analysis
assessed the effectiveness of community/school based sore throat intervention programmes in Auckland, Hawaii, the United
States and Cuba, and found, that on average, they reduced rates of ARF by 60%.19
In recent years, there have been several school-based initiatives in New Zealand. In the Northland community of Kaeo,
Whangaroa, pre-intervention rates of ARF in children aged five to 14 years were 424 per 100 000. In the eight years following
the intervention programme, which started in 2002, there have been no reported cases of ARF.
For further information see: “Why
we still need to think of rheumatic fever”, BPJ 13 (May, 2008).
The success of the Whangaroa programme has resulted in the launch of other school-based programmes. In October 2009
a similar project was launched in Opotiki.
Details of the Opotiki programme included:
- Contacting GPs before the launch to gain support and provide guidance
- Swabbing children with sore throats three times a week to ensure no more than nine days passed between onset and
treatment
- Referral of all children with positive cultures to a medical centre
- Oral antibiotics for ten days for all GAS positive students
- Raising specific community awareness of the link between sore throats and ARF
For several weeks in October 2009, when the programme started, 20% of all children with sore throats tested positive
for GAS. By December 2009 the rate had dropped to 11% and further decreased to 3% by December 2010. Identical programmes
have been launched in Kawarau (February 2011) and Murupara (May 2011).
Whānau Ora - Community solutions for community problems
In another example of forward thinking, the Mangere Community Health Trust PHO is overseeing the introduction of instant,
on-the-spot, GAS testing at Makaurau Marae, Mangere. Trust Chair, Dr Michael Lamont explains:
“A major reason why some communities have high rates of ARF is that the chain of events from sore throat to
antibiotic administration is much too long. The chain can be broken at any point, resulting in the child missing treatment.
Our solution is to do ‘near patient testing’ in the community and to make swabbing a simple and easy choice.
The old saying – make the decision the easiest and simplest thing to do!"
The GAS throat swab we have imported is 100% sensitive and 100% specific.20 It will be used on a marae in
Mangere where many of the Kuia are on their second set of heart valves.”
Sore throats break hearts
Community programmes are not just about swabbing children’s throats. Increasing community understanding of the
link between GAS sore throats and ARF is also a key component of their success. In Bay of Plenty, a multi-media campaign
was launched with locally-affected children fronting local campaigns. Press releases, advertorials and commissioned articles
appeared in newspapers, radio adverts were aired on eight stations, newsletters distributed at schools and a rheumatic
fever website created. Rheumatic fever presentations for local GPs were also conducted at CME sessions. In larger metropolitan
areas, or in sparsely populated regions where school-based projects are impractical, this raising of specific community
awareness assumes even greater significance.

In the 2011 Budget the Government announced an additional $12 million in funding allocated to combating ARF. It is
anticipated that more school-based programmes and supporting multi-media campaigns will be created. GPs in high to medium
risk areas may be asked to support such programmes as this increased funding becomes available.
Examples of the media campaigns can be seen at: www.toiteorapublichealth.govt.nz/sitesearch/?k=rheumatic+fever.
Further resources
New Zealand guidelines and educational materials are available from the National Heart Foundation website:
Acknowledgement
Thank you to Professor Norman Sharpe, Director, National Heart Foundation and Dr Jim Miller,
Medical Officer of Health and Lindsay Lowe, Communicable Disease Nurse, Toi Te Ora Public Health Service,
Bay of Plenty DHB for expert guidance in developing this article.
References
- Public Health Surveillance. Annual Surveillance Summary. Ministry of Health, 2011. Available from: www.surv.esr.cri.nz/surveillance/annual_surveillance.php (Accessed
Jul, 2011).
- Hale M, Sharpe N. Persistent rheumatic fever in New Zealand - a shameful indicator of child health. N Z Med J 2011;124(1329):6-8.
- Jaine R, Baker M, Venugopal K. Epidemiology of acute rheumatic fever in New Zealand 1995-2005. J Paediatric Child
Health 2008;44:564-71.
- The National Heart Foundation of New Zealand. New Zealand guidelines for rheumatic fever: 1 Diagnosis, management
and secondary prevention. Heart Foundation, 2006. Available from: www.heartfoundation.org.nz (Accessed
Jul, 2011).
- Kerdemelidis M, Lennon D, Arroll B, Peat B. Guidelines for sore throat management in New Zealand. N Z Med J 2009;122(1301):10-8.
- Yang LPH, Eriksson BKG, Harrington Z, et al. Variations in the protective immune response against streptococcal superantigens
in populations of different ethnicity. Med Microbiol Immunol 2006;195:37-43.
- McNicholas A, Lennon D, Crampton P, Howden-Chapman P. Overcrowding and infectious diseases - when will we learn the
lessons of our past? N Z Med J 2000;113:453-4.
- Howie JG, Foggo BA. Antibiotics, sore throats and rheumatic fever. J R Coll Gen Pract 1985;35(274):223-4.
- Carapetis JR, Currie BJ, Mathews JD. Cumulative incidence of rheumatic fever in an endemic region: a guide to the
susceptibility of a population. Epidemiol Infect 2000;124:239-44.
- Loring B. Rheumatic fever in the Bay of Plenty and Lakes District Health Boards: A review of the evidence and recommendations
for action. 2008. Available from: www.toiteorapublichealth.govt.nz/Rheumatic_Fever_GP (Accessed
Jul, 2011).
- Robson B, Hauroa RH. Māori standards of health IV. A study of the years 2000-2005. Ministry of Health,Wellington;
2007.
- The National Heart Foundation of New Zealand. Guidelines for rheumatic fever: proposed rheumatic fever primary prevention
programme. 2009. Available from: www.heartfoundation.org.nz (accessed
May, 2011).
- Lennon D, Kerdemelidis M, Arroll B, Sharpe N. Once-daily amoxicillin for Group A Streptococcal (GAS) sore throat
as the other first-line option: a clarification of the NZ sore throat guidelines. N Z Med J 2011;124(1338).
- The National Heart Foundation of New Zealand. Algorithm 4: Guide for sore throat management, 2009. Available from: www.heartfoundation.org.nz (Accessed
Jul, 2011).
- White H, Walsh W, Brown A, et al. Rheumatic heart disease in indigenous populations. Heart Lung Circ 2010;19:273-81.
- Atatoa-Carr P, Lennon D, Wilson N. Rheumatic fever diagnosis, management and secondary prevention. N Z Med J 2008;121(1271):59-69.
- Spinetto H, Lennon D, Horsburgh M. Rheumatic fever recurrence prevention: A nurse-led programme of 28 penicillin
in an area of high endemnicity. J Paediatric Child Health 2011;47(4):228-34.
- Grayson S, Horsburgh M, Lennon D. An Auckland regional audit of the nurse-led rheumatic fever secondary prophylaxis
programme. N Z Med J 2006;119(1243):U2255.
- Lennon D, Kerdemelidis M, Arroll B. Meta-analysis of trials of streptococcal throat treatment programmes to prevent
rheumatic fever. Pediatr Infect Dis 2009;28(7):e259-64.
- Scandinavian Evaluation of Laboratory Equipment for Primary Health Care. Dtec Streptococcus A test card - Strep A
test evaluation in a hospital laboratory as commissioned by Dtec AS, Norway, 2004. Available from: www.skup.nu/GetFile.ashx?fileid=325 (Accessed
Jul, 2011).