Published: 31st January, 2025 | Updated: 12th August, 2025
What's changed?
12 August 2025
Link added to commentary on LDL-C monitoring
7 July 2025 Footnote about GLP-1 receptor agonist funding restrictions removed
21 March 2025 Added clarification on concurrent use of Nicorandil with NSAIDS and aspirin
If you would like to know what changes were made when the article was updated please contact us
Key practice points
- For patients presenting with current or recent chest discomfort, confirm their symptom history, perform a clinical examination, identify any co-morbidities or risk factors that could explain their symptoms and arrange standard testing, e.g. 12-lead electrocardiogram (ECG), relevant laboratory investigations including full blood count and troponin. This evaluation process can be used to:
- Identify patients with acute chest pain red flags who require emergency department referral
- Determine the patient’s symptom origin, i.e. exclude non-cardiac causes
- Rule out other types of cardiac dysfunction, if possible, e.g. aortic stenosis
- Establish a suspected diagnosis of angina
- Refer all patients with suspected angina for non-acute cardiology assessment, but this should not delay initiating treatment in primary care
- Establish pharmacological secondary prevention including initiating an antiplatelet medicine (e.g. aspirin) and starting or optimising a lipid-lowering medicine (i.e. statin) to reduce the probability of future cardiovascular events
- The presence of co-morbidities will determine other medicines appropriate for secondary prevention, e.g. angiotensin-converting enzyme (ACE) inhibitors (or angiotensin-II receptor blockers; ARB) in patients with hypertension or chronic kidney disease
- Medicines to control angina symptoms should also be initiated
- A beta blocker or calcium channel blocker are first-line options for sustained symptomatic management. These can also be used in combination if initial monotherapy does not adequately relieve symptoms.
- Long-acting nitrates can be used as monotherapy if first-line options are not tolerated, or prescribed in addition to first-line options if symptoms are not adequately controlled
- Glyceryl trinitrate spray can be used initially for acute symptom relief
- Lifestyle changes should be discussed regularly during follow up, e.g. reducing salt and saturated fat intake, regular exercise, smoking cessation (if relevant)
- Referral for revascularisation via either percutaneous coronary intervention (PCI) or coronary-artery bypass graft (CABG) surgery should be considered for symptom control in patients who have not responded to optimal pharmacological treatment and those who are found to have extensive multivessel disease
- Invasive treatment may also have a prognostic benefit in those at highest risk of negative outcomes
What’s changed?
This is a revision of a previously published article Medical management of stable angina pectoris (BPJ 39, October, 2011). Changes include:
- A general article revision based on updated international coronary artery disease guidelines
- Information added on ischaemia with no obstructive coronary artery disease (INOCA)
- New sections on the clinical diagnosis and ongoing monitoring of stable angina
- Review of evidence comparing revascularisation with optimal pharmacological treatment
Angina pectoris is chest pain or discomfort due to transient myocardial ischaemia occurring when cardiac oxygen supply cannot meet demand.1 Stable angina is defined by predictable or reproducible symptoms that are relieved with rest or sublingual glyceryl trinitrate (Figure 1).1 In contrast, unstable angina occurs at rest (or with minimal exertion) and is considered an acute coronary syndrome.2 Unstable angina can be distinguished from other acute coronary syndromes by the absence of significantly elevated serum troponin.2 Transient myocardial ischaemia does not typically result in myocardial cell death; only minor or negligible cardiac troponin elevation is observed (see: “Recommended laboratory investigations”).2
The understanding of angina pathophysiology is changing
Previously, stable angina was thought to exclusively result from atherosclerotic plaques forming in the medium and large coronary arteries narrowing the vascular lumen over time and reducing blood flow to the myocardium, i.e. obstructive coronary artery disease (Figure 1).1 Stable angina can progress to unstable angina if there is a rupture of the obstructive plaque, and subsequent thrombosis, leading to acute blood flow restriction and myocardial ischaemia.1 Other conditions that cause or exacerbate ischaemia may also contribute to angina symptoms, e.g. aortic stenosis, atrial fibrillation, hypertrophic cardiomyopathy, pulmonary hypertension, thyrotoxicosis.1, 3
The understanding of the aetiology of stable angina is now changing.4 People who experience angina symptoms often have little or no evidence of significant coronary artery narrowing.5, 6 This phenomenon has given rise to the concept of ischaemia with no obstructive coronary artery disease (INOCA), a collection of conditions where blood flow to cardiac tissues is restricted in the absence of obvious epicardial blood flow obstruction (on coronary angiogram).5 INOCA is more commonly diagnosed in females (50 – 70%) than males (30 – 50%) who undergo coronary angiography.4, 5 The absence of overt macrovascular stenosis does not mean the INOCA is benign; patients with angina symptoms and no evidence of coronary artery disease are at higher risk of delayed diagnosis leading to more frequent hospital admission and invasive testing (e.g. coronary angiography), adverse effects, disability and poor quality of life.4, 5 The term angina with no obstructive coronary artery disease (ANOCA) is used when ischaemia has not yet been identified with stress testing.7
INOCA can manifest as:5
- Microvascular angina – Coronary microvascular dysfunction where the smallest heart vessels are either unable to vasodilate when required (e.g. during exertion) or blood flow is restricted due to vasospasm (at rest) causing angina symptoms.7 Structural changes affecting the lumen of these small vessels further increases resistance and may also contribute to endothelial dysfunction and blood flow restriction. Microvascular dysfunction is associated with conventional cardiovascular risk factors (e.g. hypertension, diabetes, dyslipidaemia) as well as chronic inflammation and mental stress.7 Microvascular angina is more common in females, potentially due to sex-specific risk factors for cardiovascular disease affecting oestrogen levels and endothelial function, e.g. menopause, premature ovarian insufficiency, polycystic ovary syndrome.7 N.B. Microvascular angina has previously been referred to as “cardiac syndrome X”.
- Vasospastic angina – Recurrent episodes of angina caused by coronary arteries on the surface of the myocardium responding abnormally (i.e. vasospasm) to circulating vasoconstrictors, e.g. acetylcholine, serotonin, histamine.8 It often occurs at rest and follows a circadian pattern (e.g. episodes overnight or in the early morning) and can be provoked by hyperventilation or exertion in some cases.8 Vasospastic angina is more common in younger people with a history of smoking.8 Conventional cardiovascular risk factors such as hypertension and diabetes may have a lesser role in the development of vasospastic angina, but its association with dyslipidaemia is uncertain.8 N.B. Prinzmetal angina is a subtype of vasospastic angina.5
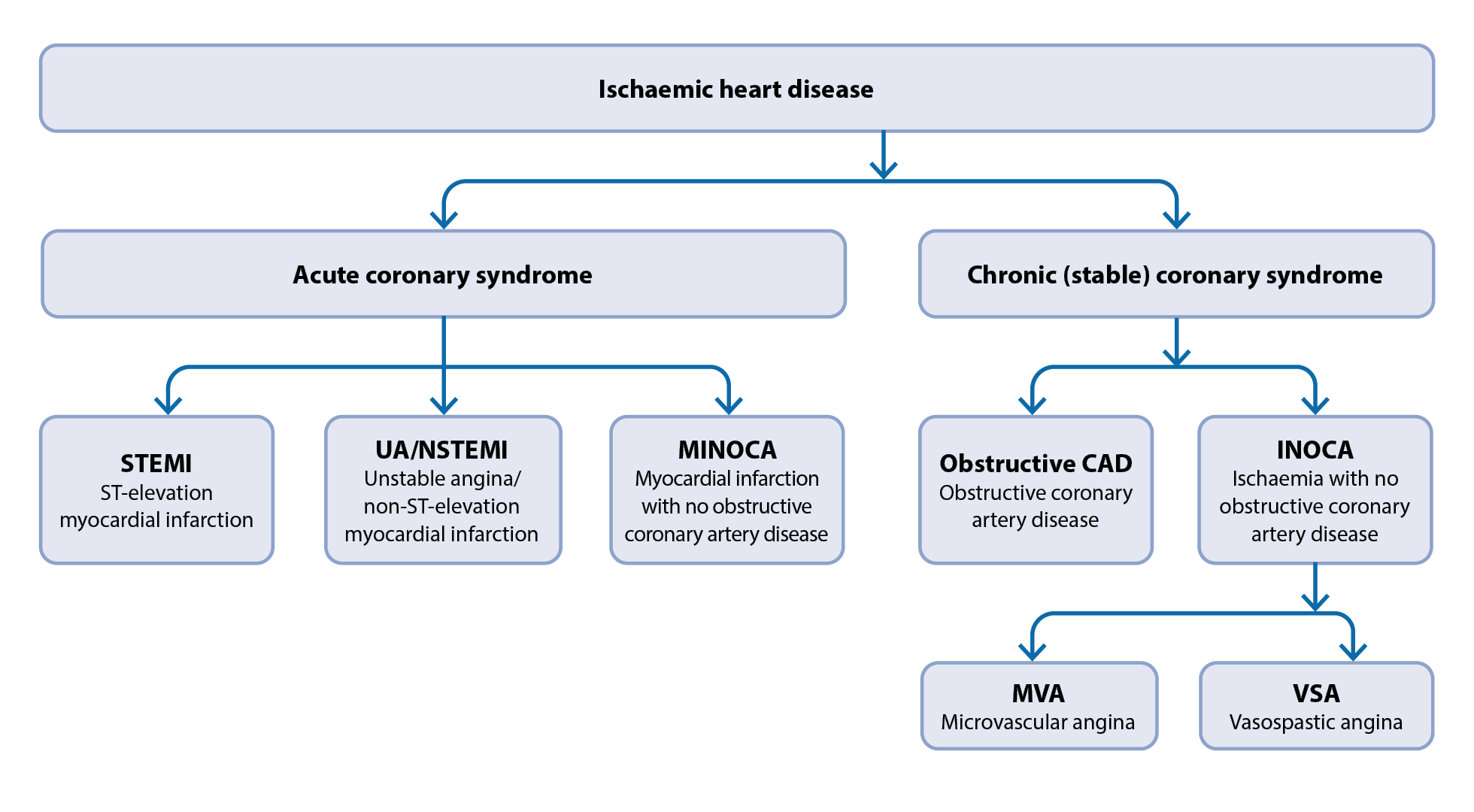
Figure 1. An overview of ischaemic heart disease.5, 9
Evaluating a patient with chest discomfort involves:4
- Ruling out acute coronary syndromes (and urgent non-cardiac causes) based on symptom history and clinical examination
- Identifying co-morbidities or risk factors that may explain symptoms or influence future management decisions
- A 12-lead electrocardiogram (ECG)
- Relevant laboratory investigations
If there is a high clinical suspicion of angina following evaluation (but no red flags – see below), initiate treatment and refer the patient for a non-acute cardiology assessment to undergo further assessment and receive a formal diagnosis.
Red flag symptoms and signs in patients requiring urgent referral for cardiology assessment
 Patients with any of the following symptoms or signs should be urgently referred to the emergency department for cardiology assessment due to the possibility of an acute coronary syndrome:2, 10
Patients with any of the following symptoms or signs should be urgently referred to the emergency department for cardiology assessment due to the possibility of an acute coronary syndrome:2, 10
- Recent (i.e. past few days) or ongoing chest discomfort:
- At rest or on minimal exertion
- Lasting longer than 15 minutes
- That is progressing rapidly despite standard treatment
- Alongside haemodynamic compromise, e.g. hypotension, tachycardia, peripheral cyanosis
- Any current changes on ECG suggesting ischaemia in a patient with new or worsening chest discomfort, including:
- ST-elevation or depression possibly indicating myocardial infarction
- Pathological Q waves indicating current (or prior) myocardial infarction
- Wellens’ sign (deeply inverted or biphasic T waves in leads V2 and V3) suggesting a critical left anterior descending coronary artery stenosis
- Left or right bundle branch block; patients presenting with bundle branch block and symptoms and signs consistent with myocardial ischaemia should be managed as if a ST-elevation myocardial infarction (STEMI) is suspected as ST changes cannot be accurately assessed
For further information on the immediate management of acute coronary syndrome in primary care, see: https://bpac.org.nz/BPJ/2015/April/coronary.aspx and https://bpac.org.nz/BPJ/2015/August/coronary.aspx (N.B. These articles are currently undergoing revision and a new version will be published in 2025.)
Establish a clinical picture based on symptom history
Angina should be suspected in patients presenting with “tight”, “dull” or “heavy” chest pain or discomfort which may be retrosternal, left-sided or difficult to localise (Table 1).1 The discomfort may also radiate to the upper arm (more commonly the left arm), neck, jaw, epigastrium or back.1, 4 Non-specific symptoms may also be reported, e.g. dyspnoea (shortness of breath), fatigue, nausea and vomiting, diaphoresis, light-headedness.4, 11 In some situations, these non-specific symptoms can be more prominent than (or reported in absence of) chest discomfort, especially in females, older adults and people with diabetes.4, 11
Symptom onset is often associated with physical exertion but other triggers include emotional stress, eating a large meal, cold weather or upon waking.4 If typical chest pain is not present, it is the association of the onset of symptoms with a trigger that increases suspicion for angina, e.g. jaw or arm pain that worsens with exercise.
Chest discomfort resulting from transient myocardial ischaemia is typically short-lived (e.g. 5 – 10 minutes); chest discomfort lasting > 15 minutes in patients with relevant symptoms should increase clinical suspicion for myocardial infarction.4, 10 Discomfort associated with stable angina typically subsides with rest (or sublingual glyceryl trinitrate; see: “Sublingual glyceryl trinitrate relieves acute symptoms of angina”), is not usually influenced by body position or respiration, and antacids and simple analgesia are unlikely to relieve symptoms (see: “Differential diagnosis of chest pain”).4, 11
Physical examination to rule out other causes
 Physical examination identifies risk factors and signs of cardiovascular disease and aids differential diagnosis (see: “Differential diagnosis of chest pain”). Measure blood pressure, heart rate and rhythm, and oxygen saturation while also taking note of the patient’s general appearance (e.g. looking for signs of distress, pallor, sweating, breathing rate and pattern).
Physical examination identifies risk factors and signs of cardiovascular disease and aids differential diagnosis (see: “Differential diagnosis of chest pain”). Measure blood pressure, heart rate and rhythm, and oxygen saturation while also taking note of the patient’s general appearance (e.g. looking for signs of distress, pallor, sweating, breathing rate and pattern).
Assess for evidence of non-atherosclerotic causes of myocardial ischaemia.1 Chest auscultation may reveal systolic murmurs suggesting aortic stenosis, hypertrophic cardiomyopathy or valvular heart disease, e.g. mitral regurgitation.2, 11 A third heart sound and bibasilar crackles in conjunction with an elevated jugular venous pressure or peripheral oedema potentially indicates congestive heart failure.12 Non-specific findings should also prompt consideration of non-cardiac conditions that underlie a reduction in myocardial oxygen supply, e.g. pallor suggesting anaemia, diaphoresis and tremor in patients with thyrotoxicosis.2
Table 1. Clinical features that may differentiate stable angina from other causes of chest discomfort.4, 10, 11
| |
Clinical features |
Increases suspicion of stable angina |
Suggestive of another cause (including unstable angina) |
Character |
How is the sensation described? |
Tight, dull or heavy chest discomfort that builds in intensity
Discomfort that is predictable (in character) and recurrent |
Sharp shooting pain or pain only felt on inspiration |
Are there any associated symptoms? |
Shortness of breath, fatigue, sweating, light headedness, nausea or restlessness |
Difficulty swallowing |
Cause |
What is the patient doing when symptoms begin? |
Physical exertion, experiencing emotional stress, has recently eaten or woken up |
Discomfort reproducible with palpation of the chest
Discomfort at rest or with minimal exertion
Positional discomfort |
Duration |
How long do symptoms last? |
Discomfort lasting minutes (e.g. 5 – 10 minutes; chest discomfort lasting > 15 minutes in patients with relevant symptoms should increase suspicion for an ACS) |
Discomfort lasting only a few seconds or that has lasted hours/days |
Location |
Where is the discomfort felt? |
Retrosternal or left-sided chest discomfort |
Discomfort primarily in the upper right quadrant of the abdomen |
Does it radiate to other parts of the body? |
Discomfort radiates to either arm, neck, jaw, epigastrium or back |
Discomfort radiates to lower extremities |
Relief |
What does it take for symptoms to go away? |
Rest (or glyceryl trinitrate; see: “Sublingual glyceryl trinitrate relieves acute symptoms of angina”) |
Repositioning, simple analgesia, antacids |
ACS = acute coronary syndrome
Differential diagnosis of chest pain
Differentiating a life-threatening cause of chest pain from a benign one in primary care can be challenging. Non-cardiac causes include gastrointestinal, musculoskeletal and respiratory conditions (Table 2).11
Table 2. Differential diagnosis of chest pain.2, 11 N.B. This is not an exhaustive list.
Cardiovascular causes |
Non-cardiac causes |
- Acute coronary syndrome
- Aortic dissection
- Myocarditis/pericarditis
- Aortic stenosis
- Mitral regurgitation
- Cardiomyopathies, e.g. dilated, restrictive or hypertrophic
|
- Gastrointestinal, e.g. gastroesophageal reflux disease, peptic ulcer disease, oesophageal spasm, oesophageal rupture
- Musculoskeletal, e.g. costochondritis
- Psychological, e.g. anxiety/panic disorder
- Respiratory, e.g. pulmonary embolism, pneumonia, pneumothorax, pneumomediastinum, malignancy
- Other, e.g. herpes zoster, severe anaemia
|
Assess cardiovascular risk factors
Clinical suspicion for angina (with underlying coronary artery disease) is increased in older patients and those with cardiovascular risk factors, e.g. hypertension, dyslipidaemia, diabetes, smoking, personal or family history of cardiovascular disease (CVD).4
Perform a resting ECG
 A resting 12-lead ECG is a standard investigation for patients presenting with chest discomfort, however, results are often normal; do not exclude a cardiac diagnosis based on a normal ECG.2, 4
A resting 12-lead ECG is a standard investigation for patients presenting with chest discomfort, however, results are often normal; do not exclude a cardiac diagnosis based on a normal ECG.2, 4
ECG findings that may potentially indicate myocardial ischaemia or obstructive coronary artery disease include:1, 4
- Repolarisation abnormalities, e.g. ST-segment elevation or depression
- Conduction abnormalities, e.g. left or right bundle branch block
- Pathological Q or R waves suggesting a previous myocardial infarction
- Other abnormalities of rate (e.g. sinus bradycardia/tachycardia) or rhythm (e.g. atrial fibrillation) or the presence of left ventricular hypertrophy
Clinicians should have a low threshold for referral in patients with chest pain; any ECG abnormality suggestive of ischaemia is typically a reason to consider acute cardiology referral. Check the patient’s medical records for previous ECG recordings as these can be used as a baseline for comparison. A discussion with a colleague (or cardiologist) can be useful if there is uncertainty regarding the appropriate management strategy, e.g. acute cardiology referral or initial treatment in primary care (with non-acute cardiology referral).
Recommended laboratory investigations
Serum troponin is the key biomarker to establish myocardial injury; a significantly elevated circulating troponin level (above the 99th percentile) in a patient with relevant symptoms and signs is diagnostic of myocardial infarction, e.g. STEMI or non-ST-elevation myocardial infarction (NSTEMI).2 Troponin levels typically rise soon after symptoms develop and can remain elevated for up to ten days following a myocardial infarction.13 Troponin testing is useful in a primary care setting to rule out an acute coronary syndrome if there is clinical uncertainty or to identify patients who have experienced a recent myocardial infarction but are now asymptomatic.13 N.B. Troponin testing is generally not necessary in patients with stable recurrent discomfort.
Collect a blood sample at initial presentation, if possible. Depending on the patient’s clinical condition, troponin levels may be assayed urgently in a community laboratory, or the blood sample can be sent with the patient to hospital.
Other laboratory tests that help build a clinical picture include:2, 4, 14
- Full blood count (specifically haemoglobin to rule out anaemia)
- Brain natriuretic peptide (BNP) if heart failure is suspected
- Lipid profile
- Electrolytes (e.g. potassium) and creatinine (and calculated eGFR)
- HbA1c
- Thyroid stimulating hormone (TSH) if there is evidence of thyroid dysfunction
- C-reactive protein (CRP) if infection is suspected
- Liver function tests (LFTs) prior to initiating a statin
A chest X-ray is not routinely recommended but may be indicated in patients who present with atypical symptoms suggesting a pulmonary origin.4 Arrange an echocardiogram if there is clinical suspicion that heart failure or valvular disease are the cause of the patient’s symptoms (however, patients with angina may experience these conditions concomitantly).1, 4
Best practice tip: Interpret elevated troponin levels in the context of the patient’s symptoms; increased serum troponin is not always associated with coronary pathology (or acute coronary syndrome).15 Examples of non-cardiac conditions where people may experience troponin elevation include chronic obstructive pulmonary disease (COPD) exacerbations, gastrointestinal bleeding, acute and chronic renal failure and sepsis.15
Refer all patients with suspected angina for cardiology assessment
 Request a non-acute cardiology assessment for all patients with suspected angina, however, this should not delay the initiation of secondary prevention or anti-ischaemic medicines.
Request a non-acute cardiology assessment for all patients with suspected angina, however, this should not delay the initiation of secondary prevention or anti-ischaemic medicines.
A formal diagnosis of stable angina is generally made in secondary care following further assessment. Depending on the patient’s clinical condition, presence of contraindications, pre-test probability of coronary artery disease and local availability of resources, they may undergo:1, 16
- Stress testing (with exercise or dobutamine)
- Echocardiography
- Computed tomography coronary angiography (CTCA) including coronary artery calcium score
- Invasive coronary angiography
- Myocardial perfusion scintigraphy using single photon emission computed tomography (SPECT)
This cardiology assessment will usually identify patients who are appropriate candidates for revascularisation or optimal pharmacological treatment alone; see: “Revascularisation may improve symptoms and prognosis”.
Give clear instructions regarding worsening symptoms
 Advise patients to seek immediate medical attention if their symptoms worsen before their next appointment. This may include an increase in symptom severity or frequency, a significant reduction in the threshold at which symptoms occur, symptoms occur at rest or symptoms that are not relieved with glyceryl trinitrate (see: “Sublingual glyceryl trinitrate relieves acute symptoms of angina”).
Advise patients to seek immediate medical attention if their symptoms worsen before their next appointment. This may include an increase in symptom severity or frequency, a significant reduction in the threshold at which symptoms occur, symptoms occur at rest or symptoms that are not relieved with glyceryl trinitrate (see: “Sublingual glyceryl trinitrate relieves acute symptoms of angina”).
Pharmacological management of stable angina has two purposes:4
- Reduce the risk of future cardiovascular events (e.g. myocardial infarction) and death with lifestyle changes and preventative medicines; and
- Improve the patient’s quality of life by alleviating symptoms with anti-ischaemic medicines
Primary care clinicians should initiate medicines for both purposes if stable angina is suspected. Further risk stratification with stress testing and angiography may be used during cardiology assessment to identify patients who are suitable for revascularisation or require modification of initial medicines. Revascularisation is usually undertaken for symptom control but also for prognostic benefit in a small subset of patients identified at angiography (see: “Revascularisation may improve symptoms and prognosis ”).4, 6
Lifestyle changes to reduce cardiovascular risk
Lifestyle changes are a key component of angina management, reducing the risk of future cardiovascular events and death.1 Individual lifestyle advice should be given to all patients with suspected stable angina and revisited during follow-up.4 Routine assessment of body mass index (BMI) and waist circumference is recommended to monitor progress and assess the efficacy of lifestyle interventions.6
Recommendations for patients with suspected angina include:6
 Reduce body weight or limit weight gain through lifestyle interventions below. Patients should target a BMI of < 25 kg/m2 or a reduction in waist circumference.
Reduce body weight or limit weight gain through lifestyle interventions below. Patients should target a BMI of < 25 kg/m2 or a reduction in waist circumference.
 Follow a healthy diet focusing on lean proteins, fruit and vegetables, legumes, nuts and whole grains. Aim to reduce calories from saturated fats (< 6% of daily calorie intake) and reduce daily sodium intake to < 1,500 mg per day (equivalent to less than one teaspoon of table salt).17
Follow a healthy diet focusing on lean proteins, fruit and vegetables, legumes, nuts and whole grains. Aim to reduce calories from saturated fats (< 6% of daily calorie intake) and reduce daily sodium intake to < 1,500 mg per day (equivalent to less than one teaspoon of table salt).17
 Increase physical activity. All patients should reduce sedentary behaviour and introduce regular physical activity based on their clinical condition, co-morbidities and physical capacity. Where possible, slowly increase weekly exercise targets until the patient can achieve exercise recommendations, i.e. 150 minutes of aerobic or 75 minutes of high intensity physical activity per week. Resistance (strength) training should also be incorporated at least two times per week, if appropriate.
Increase physical activity. All patients should reduce sedentary behaviour and introduce regular physical activity based on their clinical condition, co-morbidities and physical capacity. Where possible, slowly increase weekly exercise targets until the patient can achieve exercise recommendations, i.e. 150 minutes of aerobic or 75 minutes of high intensity physical activity per week. Resistance (strength) training should also be incorporated at least two times per week, if appropriate.
 Reduce daily alcohol consumption. New Zealand guidelines recommend to not exceed a daily limit of three standard drinks for males and two standard drinks for females, and have at least two alcohol-free days per week, however, no level of alcohol consumption is considered to be without risk.18 Do not recommend alcohol to reduce a patient’s risk of CVD (e.g. a glass of red wine for “heart health”) as there is no good evidence to support this.18
Reduce daily alcohol consumption. New Zealand guidelines recommend to not exceed a daily limit of three standard drinks for males and two standard drinks for females, and have at least two alcohol-free days per week, however, no level of alcohol consumption is considered to be without risk.18 Do not recommend alcohol to reduce a patient’s risk of CVD (e.g. a glass of red wine for “heart health”) as there is no good evidence to support this.18
 Smoking cessation using behavioural and pharmacological interventions, e.g. nicotine replacement therapy. Passive exposure to tobacco smoke should also be avoided.
Smoking cessation using behavioural and pharmacological interventions, e.g. nicotine replacement therapy. Passive exposure to tobacco smoke should also be avoided.
 Identify and address any mental health concerns that may influence cardiovascular outcomes. Use pharmacological and non-pharmacological management options as appropriate.
Identify and address any mental health concerns that may influence cardiovascular outcomes. Use pharmacological and non-pharmacological management options as appropriate.
Consider referral to a cardiac rehabilitation programme
Cardiac rehabilitation is a cardiac-focused, multidisciplinary support programme that provides education and aids lifestyle changes to improve outcomes in people with CVD.6 It may also involve supervised group exercise, peer group support and social events. Cardiac rehabilitation is recommended for all patients with stable angina.6 Advise patients there may be a cost associated with some programmes.
For a list of cardiac rehabilitation programmes throughout New Zealand, see: https://hhdirectory.heartfoundation.org.nz/
For further information on weight loss, alcohol and smoking cessation, see:
Pharmacological options to prevent future cardiovascular events
Cardiovascular event risk can be reduced with pharmacological intervention (Table 3). All patients with suspected stable angina should be prescribed the following medicines for prevention of future cardiovascular events:6
- Antiplatelet (e.g. aspirin, clopidogrel), unless contraindicated
- Statin, e.g. atorvastatin
Medicines that may be considered depending on co-morbidities include:4, 6
- Angiotensin-converting enzyme (ACE) inhibitor or angiotensin-II receptor blocker (ARB)
- Sodium-glucose co-transporter 2 (SGLT-2) inhibitor (e.g. empagliflozin) or glucagon-like peptide 1 (GLP-1) receptor agonist, e.g. dulaglutide, liraglutide
Table 3. Pharmacological options to reduce the long-term risk of cardiovascular events.4, 6, 19, 20
Medicine |
Indications |
Recommended dosing |
Aspirin (or clopidogrel) |
Prescribe to all patients without contraindications or co-morbidities to reduce thrombosis risk |
Aspirin 75 – 150 mg, once daily (or clopidogrel 75 mg, once daily) |
Statin |
Prescribe to all patients, regardless of LDL-C, aiming to achieve a target of < 1.4 mmol/L and a ≥ 50% reduction from baseline |
Initially atorvastatin 10 – 40 mg, once daily (then adjust dose depending on the patient’s LDL-C response); maximum 80 mg, once daily
N.B. Rosuvastatin can be prescribed first-line with Special Authority approval for Māori and Pacific peoples at risk of CVD and second-line in patients who cannot achieve LDL-C targets with optimal atorvastatin or simvastatin treatment. |
ACE inhibitor (or ARB) |
Patients with co-existing indications for ACE inhibitors, e.g. hypertension, diabetes, heart failure with LVEF ≤ 40%, chronic kidney disease |
See NZF for specific dosing
|
SGLT-2 inhibitor (or GLP-1 receptor agonist) |
Patients with co-existing type 2 diabetes or heart failure |
See NZF for specific dosing
|
ACE inhibitor = Angiotensin-converting enzyme inhibitor, ARB = Angiotensin-II receptor blocker, CVD = cardiovascular disease, GLP-1 receptor agonist = Glucagon-like peptide 1 receptor agonist, LDL-C = Low-density lipoprotein cholesterol, LVEF = Left ventricular ejection fraction, SGLT-2 inhibitor = Sodium-glucose co-transporter 2 inhibitor
Prescribe aspirin or another antiplatelet
Aspirin should be prescribed to most patients with stable angina (Table 3).6 Consider bleeding risk before prescribing aspirin in patients with a history of peptic ulcer disease.19 A proton pump inhibitor (PPI; e.g. omeprazole) can be prescribed if aspirin is indicated in patients at elevated risk of gastrointestinal bleeding.4 Aspirin should not be prescribed to patients with:6, 19
- Hypersensitivity to aspirin (or any other NSAIDs)
- Haemophilia
- An indication for anticoagulation, e.g. concomitant atrial fibrillation, history of deep vein thrombosis, pulmonary embolism
Antiplatelet treatment with aspirin leads to a significant reduction in serious vascular events, non-fatal myocardial infarction, non-fatal stroke and vascular mortality in people with CVD, including those with stable angina.4, 21
Clopidogrel is an alternative antiplatelet medicine for patients who cannot tolerate aspirin or in whom aspirin is contraindicated.4 Aspirin and clopidogrel are prescribed together for between 1 – 12 months in patients who have undergone percutaneous coronary intervention (PCI) for angina symptoms or following an acute coronary syndrome.4 Antiplatelet treatment is then switched to a single medicine long term to reduce the risk of major adverse cardiovascular effects (see: “Revascularisation may improve symptoms and prognosis”).4 Gastroprotection may still be required depending on the patient’s bleeding risk (see note below).
N.B. Due to a theoretical interaction between omeprazole and clopidogrel (omeprazole inhibits the enzyme that metabolises clopidogrel), this combination should be avoided.4 Lansoprazole or pantoprazole can be considered if a PPI is required during clopidogrel monotherapy.4
All patients with stable angina should be taking a statin
Statins are strongly recommended in patients with angina, regardless of baseline LDL-C, as they are considered to have a five-year CVD risk of > 15% (Table 3).4, 22 High potency statin treatment, e.g. atorvastatin 40 – 80 mg or rosuvastatin 10 – 40 mg, reduces the risk of major cardiovascular events by approximately 15%, compared to moderate-intensity statin treatment in patients with acute coronary syndrome or stable coronary disease.6, 23 This benefit is more likely to be experienced by people with higher LDL-C levels at baseline.6, 23 Consider adjuvant medicines (e.g. ezetimibe) in patients who cannot reach the target LDL-C level (i.e. < 1.4 mmol/L) with the maximum recommended dose of a high potency statin.6, 20
Do not prescribe fibrates (e.g. bezafibrate), nicotinic acid derivatives (e.g. acipimox) or omega-3 fatty acid supplements to patients already taking a statin as there is unlikely to be any further reduction in cardiovascular risk.6
For further information on prescribing statins to reduce cardiovascular risk, see: https://bpac.org.nz/2021/statins.aspx and https://bpac.org.nz/2022/rosuvastatin.aspx
ACE inhibitors or ARBs are recommended for patients with pre-existing indications for their use
It is unclear if an ACE inhibitor or ARB is of benefit in the management of stable angina.4 Current evidence suggests ACE inhibitors may not improve symptoms or long-term prognosis in people with stable angina and no other cardiovascular risk factors, therefore they are generally only recommended for patients with pre-existing conditions that would benefit from their use, e.g. hypertension, heart failure, chronic kidney disease.4 Patients with coronary artery disease are likely to experience similar outcomes regardless of whether they are prescribed ACE inhibitors or ARBs.24 Clinical situations where an ARB may be preferred include for patients who are intolerant to ACE inhibitors or who have a reduced eGFR.24
The Women’s IschemiA TRial to Reduce Events In Non-ObstRuctive CAD (WARRIOR) trial is currently underway and the results are expected to provide a more definitive conclusion; this multicentre randomised controlled trial compares the effect of intensive treatment (including an ACE inhibitor or ARB) with standard primary prevention in the development of major adverse coronary events over approximately three years in more than 4,000 female participants with symptomatic INOCA.25 The results are expected to be published soon.
For further information on the appropriate management of hypertension, heart failure and chronic kidney disease, see:
Consider SGLT-2 inhibitors or GLP-1 receptor agonists in patients with stable angina to reduce cardiovascular risk
Guidelines recommend the use of a SGLT-2 inhibitor or a GLP-1 receptor agonist in patients with coronary artery disease (and stable angina) and type 2 diabetes because of the associated reduction of future cardiovascular morbidity and mortality.4, 6 In addition, SGLT-2 inhibitors are now recommended for patients with heart failure with a reduced ejection fraction (HFrEF), heart failure with a preserved ejection fraction (HFpEF) or heart failure and chronic kidney disease, regardless of diabetes status, and should be considered in patients with stable angina and any of these co-morbidities.6, 26, 27
In New Zealand, empagliflozin (a SGLT-2 inhibitor) is funded with Special Authority approval for patients with type 2 diabetes and as of 1st December, 2024, also those with HFrEF. GLP-1 receptor agonists are currently only funded with Special Authority approval for patients with type 2 diabetes.
Ongoing management of angina symptoms
 Beta blockers or calcium channel blockers are generally recommended as first-line options for preventing angina symptoms.4 They can be prescribed in combination in patients whose symptoms are not controlled with a single medicine and who are not suitable for revascularisation.4 A long-acting nitrate can also be added to a beta blocker or calcium channel blocker if symptoms are not controlled, or used as monotherapy in some situations such as if first-line medicines are contraindicated or adverse effects are intolerable.4 All three of these medicines can help to reduce symptoms (e.g. fewer angina episodes, improved exercise duration), and no option is considered superior to another in the management of angina.28 Therefore, medicine selection is dependent on the patient’s clinical condition, co-morbidities, potential for medicines interactions, adherence, and preferences (e.g. dose frequency, potential adverse effects).4 For example, prescribe beta blockers in patients with a high resting heart rate, previous myocardial infarction or HFrEF, whereas calcium channel blockers are preferred in patients with vasospastic angina, asthma or COPD.3, 29 Figure 2 provides a summary of funded medicines available for managing angina symptoms in primary care in New Zealand.
Beta blockers or calcium channel blockers are generally recommended as first-line options for preventing angina symptoms.4 They can be prescribed in combination in patients whose symptoms are not controlled with a single medicine and who are not suitable for revascularisation.4 A long-acting nitrate can also be added to a beta blocker or calcium channel blocker if symptoms are not controlled, or used as monotherapy in some situations such as if first-line medicines are contraindicated or adverse effects are intolerable.4 All three of these medicines can help to reduce symptoms (e.g. fewer angina episodes, improved exercise duration), and no option is considered superior to another in the management of angina.28 Therefore, medicine selection is dependent on the patient’s clinical condition, co-morbidities, potential for medicines interactions, adherence, and preferences (e.g. dose frequency, potential adverse effects).4 For example, prescribe beta blockers in patients with a high resting heart rate, previous myocardial infarction or HFrEF, whereas calcium channel blockers are preferred in patients with vasospastic angina, asthma or COPD.3, 29 Figure 2 provides a summary of funded medicines available for managing angina symptoms in primary care in New Zealand.
For further information on specific medicines and dosing information, see: https://nzf.org.nz/nzf_1550

Figure 2. Summary of funded medicines available for managing angina symptoms in primary care in New Zealand.4, 19, 29 N.B. Perhexiline, only prescribed under specialist supervision, and ivabradine, not funded, are available in New Zealand but have not been included in this figure.
* Diltiazem can be considered in combination with beta blockers in some cases (caution is advised; see: “Consider prescribing both a beta blocker and a calcium channel blocker”)
Beta blockers improve angina symptoms by reducing heart rate and myocardial contractility and decreasing blood pressure.4, 29 The combined result is a reduction in myocardial oxygen demand at rest and during exertion.29 Beta blockers have not specifically been shown to reduce mortality in people with stable angina but there is evidence of improved prognosis in those who have previously had a myocardial infarction or have HFrEF.4, 29 Treatment efficacy is likely similar, irrespective of receptor subtype selectivity, however, cardioselective beta blockers (e.g. bisoprolol, metoprolol and atenolol) may be more tolerable.30
Beta blockers are contraindicated in patients with vasospastic angina as they may promote coronary vasospasm.29
Calcium channel blockers minimise symptoms of angina by dilating coronary arteries reducing vessel resistance and left ventricular afterload.29 Non-dihydropyridine calcium channel blockers (e.g. verapamil and diltiazem) also reduce myocardial contractility and heart rate, and decrease myocardial oxygen demand.* 29 There is no evidence of difference in exercise duration or exercise time to angina between patients taking beta blockers or calcium channel blockers.28
A calcium channel blocker may be preferred for patients in whom a beta blocker is contraindicated or is not tolerated. Long-acting calcium channel blockers (e.g. amlodipine) or modified-release formulations should be prescribed; short-acting dihydropyridine calcium channel blockers are not recommended because they may cause reflex tachycardia exacerbating myocardial ischaemia.29
* Avoid prescribing verapamil and diltiazem to patients with left ventricular dysfunction, bradycardia or conduction disturbances29
Consider prescribing both a beta blocker and a calcium channel blocker
Prescribe a beta blocker with a non-rate limiting (dihydropyridine) calcium channel blocker (e.g. felodipine or amlodipine), if required.4, 31 In some cases, diltiazem can be considered in combination with beta blockers (caution is advised), however, it should be avoided in patients with left ventricular dysfunction (i.e. left ventricular ejection fraction [LVEF] < 40%, HFrEF) due to the risk of left ventricular failure and severe bradycardia.4, 6 Avoid verapamil in combination with a beta blocker as there is an increased risk of heart block.4
Use long-acting nitrates in combination with first-line options
Long-acting nitrates (e.g. isosorbide mononitrate) may be added to a beta blocker or calcium channel blocker in patients who do not have an adequate response to maximum tolerated doses.4 They are also appropriate if first-line medicines are contraindicated or not tolerated.4 Nitrates produce venous and arterial dilation, reducing ventricular pre-load and after-load which lowers myocardial oxygen demand and improves subendocardial blood flow.29
Tolerance is a major concern with prolonged use of long-acting nitrates reducing their efficacy.4 A “nitrate-free” interval of 8 – 10 hours is required each day to avoid this.4
Trial nicorandil in patients with refractory angina
Nicorandil is a potassium channel activator with nitrate-like effects that promotes coronary and peripheral vasodilation.32 It can be used as a monotherapy, or in combination with other anti-ischaemic medicines, if symptoms are not well controlled.4 In contrast to nitrates, tolerance to the vasodilatory effects of nicorandil is not expected with long-term dosing.32 Cross-tolerance with nitrates is also unlikely.32 In rare cases, people taking nicorandil have developed gastrointestinal, mucosal, cutaneous or ocular ulcers.33 This can occur at any time during treatment, e.g. years after starting treatment.33 Patients should be advised to immediately stop treatment if symptoms develop.32, 33The risk of gastrointestinal ulceration is increased with concurrent use of nicorandil with NSAIDs or aspirin*,33 therefore this combination should be prescribed with caution and the patient closely monitored for adverse effects. Many patients with angina will be taking low-dose aspirin – there is no specific information on what to do in this situation if they require nicorandil (other than to balance the risks and benefits), but a pragmatic approach may be to add a PPI if they are not already taking one.
* This caution does not differentiate between antiplatelet and analgesic doses; see Nicorandil Summary of Product Characteristics UK (2017)
Perhexiline, another option for refractory angina, increases fatty acid oxidation in the myocardium improving metabolic efficiency.34 This medicine should only be prescribed under specialist supervision.19 Therapeutic dose monitoring is required as perhexiline is associated with significant adverse effects, e.g. neuropathy.19
Sublingual glyceryl trinitrate relieves acute symptoms of angina
Prescribe sublingual glyceryl trinitrate spray to patients for use at the onset of symptoms while optimising anti-ischaemic medicine dosing.4 It may also be used before activities that are known to trigger angina symptoms, e.g. exercise, sexual intercourse*.4 Advise patients to use the spray while seated due to the risk of postural hypotension and syncope.19 Other adverse effects include facial flushing and headaches;19 instruct patients to return for evaluation if these become severe.
* Concomitant use of glyceryl trinitrate with a phosphodiesterase type-5 inhibitor is contraindicated due to the risk of severe hypotension19
Further information for patients, including an angina action plan, is available from: https://www.heartfoundation.org.nz/your-heart/heart-conditions/angina
Inequities in glyceryl trinitrate dispensing
The exact prevalence of stable angina in New Zealand is unknown, however, it can be inferred based on the dispensing of sublingual glyceryl trinitrate spray, which is recommended for acute symptomatic relief in all patients with stable angina. Approximately 50,000 patients were prescribed glyceryl trinitrate in 2023.35 The rate of glyceryl trinitrate dispensing increased with age (Figure 3A), reflecting the higher prevalence of ischaemic heart disease in older adults.36
The rate of glyceryl trinitrate dispensing varies by ethnicity (Figure 3B). Current dispensing data suggests that people of European/Other ethnicity are prescribed glyceryl trinitrate more often than Māori and Pacific peoples.35 Given that evidence shows Māori and Pacific peoples experience a higher CVD burden (including ischaemic heart disease), compared to people of European ethnicity,37 these results potentially indicate under-recognition (or under-reporting) of angina symptoms in these groups.
Figure 3. Dispensing of glyceryl trinitrate by (A) age and (B) ethnicity (number of patients with at least one dispensing per 1,000 population) in New Zealand in 2023.35 Note the different scales on the y-axis between panels A and B.
Optimise treatment through regular monitoring
Regular follow-up and monitoring are required for patients with stable angina to prevent disease progression. This includes symptom control prior to cardiology assessment, medicines optimisation and the long-term monitoring and management of CVD risk factors.
 Medicines optimisation. Evaluate the patient’s clinical response and any adverse effects two to four weeks after starting anti-ischaemic medicines.1 Depending on the frequency and severity of the patient’s symptoms, a second (or third) medicine may need to be initiated.6 Patients with refractory symptoms despite maximum tolerated doses of anti-ischaemic medicines should be discussed with a cardiologist as more invasive management may be required, i.e. revascularisation.
Medicines optimisation. Evaluate the patient’s clinical response and any adverse effects two to four weeks after starting anti-ischaemic medicines.1 Depending on the frequency and severity of the patient’s symptoms, a second (or third) medicine may need to be initiated.6 Patients with refractory symptoms despite maximum tolerated doses of anti-ischaemic medicines should be discussed with a cardiologist as more invasive management may be required, i.e. revascularisation.
Re-check the patient’s lipid profile at 12 weeks to assess their response to high-intensity statin treatment and optimise LDL-C-lowering treatment, if required.6
For commentary on LDL-C monitoring in patients with established cardiovascular disease, see: “Paper of the Week: Optimising LDL-C post-ACS – is there room for improvement”, Best Practice Bulletin 129, Aug, 2025
 Long-term monitoring. Regular follow-up is recommended for all patients with stable angina, even if asymptomatic, however, the exact frequency is unclear and should be determined by the patient’s clinical condition.4 Annual review is usually appropriate for stable patients, whereas those with poorly controlled symptoms, multiple co-morbidities or newly diagnosed should undergo evaluation every six months or sooner. Review treatment response and symptom stability, lifestyle modifications (including BMI), medicines adherence and cardiovascular risk profile at follow-up.4 Carry out an ECG and arrange relevant laboratory testing including full blood count, HbA1c, creatinine (for renal function), electrolytes and lipid profile.4 A recurrence of angina symptoms following a period of successful management (with either medicines or revascularisation) is suggestive of coronary artery disease progression; referral for further non-acute cardiology assessment is recommended.
Long-term monitoring. Regular follow-up is recommended for all patients with stable angina, even if asymptomatic, however, the exact frequency is unclear and should be determined by the patient’s clinical condition.4 Annual review is usually appropriate for stable patients, whereas those with poorly controlled symptoms, multiple co-morbidities or newly diagnosed should undergo evaluation every six months or sooner. Review treatment response and symptom stability, lifestyle modifications (including BMI), medicines adherence and cardiovascular risk profile at follow-up.4 Carry out an ECG and arrange relevant laboratory testing including full blood count, HbA1c, creatinine (for renal function), electrolytes and lipid profile.4 A recurrence of angina symptoms following a period of successful management (with either medicines or revascularisation) is suggestive of coronary artery disease progression; referral for further non-acute cardiology assessment is recommended.
Revascularisation may improve symptoms and prognosis
Revascularisation involves either percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG) surgery,31 and is typically recommended for symptom control in patients who continue to experience angina despite optimal pharmacological treatment.4 Invasive intervention strategies are also recommended in those at highest risk of negative outcomes as they may improve survival in this group, e.g. patients with symptomatic multi-vessel disease, proximal left anterior descending or left main artery disease, left ventricular systolic dysfunction.6 This is in contrast to STEMI/NSTEMI management, where reperfusion via revascularisation improves survival and should be considered for most patients, depending on their clinical status and co-morbidities.2, 38
Secondary prevention measures must be continued as revascularisation does not prevent coronary artery disease progression. Previously non-obstructive plaques can develop into high-grade stenosis causing myocardial ischaemia after a symptom free period.39 Repeat revascularisation may be necessary after PCI or CABG but is more common after PCI.40
Optimal pharmacological treatment or revascularisation?
Based on the available evidence, it is unlikely revascularisation significantly reduces morbidity and mortality compared to optimal pharmacological treatment in most patients with stable coronary artery disease.41 The Clinical Outcomes Utilising Revascularization and Aggressive Drug Evaluation (COURAGE) trial (2007) and the Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) trial (2009) compared revascularisation and optimal pharmacological treatment against medical treatment alone in different patient groups.42, 43 Overall, there were no significant differences in the risk of death or major cardiovascular events.42, 43 One possible explanation for this was that both studies excluded participants with moderate-to-severe coronary artery disease or high-risk anatomical features who may have been more likely to benefit from invasive management.
In 2020, the International Study of Comparative Health Effectiveness with Medical and Invasive Approaches (ISCHEMIA) trial involved more than 5,000 participants from 37 countries with moderate or severe coronary artery disease determined by non-invasive testing.44 Participants were randomised to receive optimal pharmacological treatment and invasive cardiac catheterisation prior to either PCI or CABG (if deemed appropriate) or optimal pharmacological treatment alone.44 The primary end point included cardiovascular death, non-fatal myocardial infarction, hospitalisation for stable angina or heart failure or resuscitated cardiac arrest.44 After 3.2 years of follow-up there was no difference in primary end point between the invasive (16.4%) and conservative (18.2%) treatment arms.44 No difference in all-cause mortality was found when follow-up was extended to a median of 5.7 years, however, the risk of cardiovascular mortality reduced in the invasive intervention group while the risk of non-cardiovascular mortality increased.45
Notably, a sub-study of the ISCHEMIA trial showed a larger self-reported improvement in angina-related health status (e.g. angina symptoms, physical function and quality of life) for participants who underwent revascularisation, compared to the conservative intervention.46 A greater effect was observed in participants with more severe angina symptoms at baseline.46





