In this article 
View / Download
pdf version of this article
He tawhiti kē to koutou haerenga Ki te kore e haere tonu
He tino nui rawa o koutou mahi Kia kore e mahi nui tonu
We have come too far not to go further, we have done too much not to do more
The PHO Performance Programme (PPP) recognises the increased health needs of Māori, Pacific peoples and those living
in lower socioeconomic areas (high needs populations).
The Programme has developed a number of performance indicators to measure PHO achievements.
While a greater financial incentive is offered for achieving targets for indicators that have a high needs component,
there have been improvements across most indicators, even after financial incentives are no longer offered.
Indicators where reliable information is specifically available for the high needs populations include:
- Cervical cancer screening coverage
- Breast cancer screening coverage
- Age appropriate vaccinations for two-year-olds
- Influenza vaccinations in people aged 65 years or over
It is thought that people with mental health problems may be represented at a lower rate across all PHO indicators.
Specific primary care initiatives should be considered to ensure these people are not only receiving appropriate mental
health care, but are also receiving other essential healthcare services.
PHO Performance Programme1
The PHO Performance Programme aims to improve the health of enrolled populations and reduce inequalities in health
outcomes, through supporting clinical governance and rewarding quality improvement processes. Its success depends on
the engagement and commitment of District Health Boards, Primary Health Organisations, providers and professional groups.
The Programme aims to:
- Encourage and reward improved performance by PHOs in line with evidence based guidelines
- Measure and reward progress in reducing health inequalities by including a focus on high needs populations
Cervical Screening
Key messages:
- Target Māori, Pacific and Asian women and women from areas of high deprivation for cervical screening
- Target women over 30 years, who have never had a smear, or have not had a smear for over five years
- Target interventions carefully to avoid increasing disparities
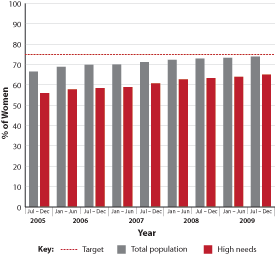 |
| Figure 1: Percentage of enrolled women aged 20–69 years who have received a cervical smear
in the past three years2 |
Programme goal
The PPP goal is for 75% or more of all women aged 20–69 years to have had cervical screening within three years.
There has been a steady increase in cervical screening rates over the past two years (Figure 1).2 However,
there is still greater improvement required and a significant gap persists between the total and high needs populations.
There is significant regional variation, with screening rates ranging from 43% to 86% for the total population and 43%
to 79% for the high needs population.3
As rates of screening have improved, the rate of cervical cancer in Māori women has fallen. However, Māori
women still have higher rates of cervical cancer than non-Māori women, and are four times more likely to die from
cervical cancer than European women.4 It is likely that suboptimal rates of screening are a major contributor
to this.
There are many barriers that may explain the reluctance of some woman to attend for cervical screening. Some are common
to all women, such as shyness or cost, while other reasons may be specific to some groups, such as cultural and language
barriers.
 See BPJ 23 (Sep, 2009) “Cervical
smears – achieving equity” for further information
See BPJ 23 (Sep, 2009) “Cervical
smears – achieving equity” for further information
Breast screening
Key messages:
- Māori and Pacific women have lower rates of breast screening and as a result, have a higher mortality rate from
breast cancer
- General practice can play a key role in addressing this inequality by ensuring all eligible women are assisted to
enrol and participate in the breast screening programme
- Practices that have made a commitment to increasing breast screening rates for Māori and Pacific women are finding
they can make significant improvements in screening rates
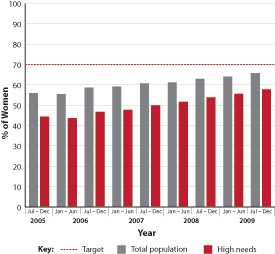 |
| Figure 2: Percentage of enrolled women aged 50 to 64 years who have received a mammogram from an
authorised provider in the past two years2 |
Programme goal
The PPP goal is for 70% or more of all high needs women aged 50 to 64 years to have had a mammogram within two years.
While this target currently measures screening rates for women aged between 50 and 64 years, in the future it will align
with the National Breast Screening Programme (i.e. 45 to 69 years).
There has been a steady increase in breast screening rates over the past two years (Figure 2).2 However,
improvement is still required, and a significant gap persists between the total and high needs populations.
There is also significant regional variation in breast screening rates, which range from 33% to 84% for the total population
and from 31% to 77% for the high needs population.3
See BPJ 24 (Nov, 2009) “Breast
Screening – achieving equity” for further information
Age appropriate vaccinations for two-year-olds
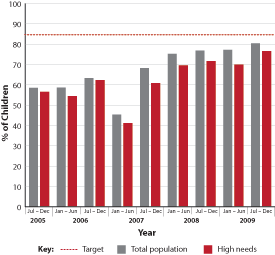 |
| Figure 3: Percentage of enrolled children aged two to three years who have received full vaccinations2 |
Programme goal
The PPP goal is for 85% or more of a PHO’s target population to have received their complete set of age appropriate
vaccinations.
Immunisation rates are increasing (Figure 3), however, again there appears to be significant regional variation with
rates ranging from 32% to 93% for the total population and 30% to 96% for the high needs population.3
Reported immunisation rates may be lower in some regions due to technical difficulties in collecting data.
Influenza vaccinations in people aged 65 years or older
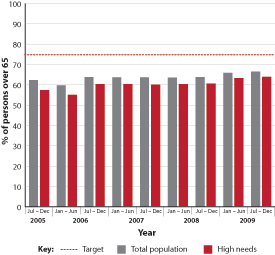 |
| Figure 4: Percentage of enrolled persons aged 65 years or older who have been vaccinated within
the flu season2 |
Programme goal
The PPP goal is for 75% or more of a PHO’s target population to have had a flu vaccination by 30 June of each
year.
Influenza vaccine coverage has remained relatively steady over the past two years, but is still below the target of
75% for all populations (Figure 4).
There is significant regional variation with influenza vaccination rates ranging from 31% to 76% for both the total
and high needs populations.3
Other indicators
There are additional indicators that are also important for the high needs population. However, data is not complete
and as a result they have not been included in this discussion. These indicators include:
Cardiovascular risk assessment
- PPP goal: 80% of the target population to have been assessed for their risk of developing cardiovascular disease.
Diabetes detection
- PPP goal: 90% of those estimated to have diabetes to have been identified and coded by their GP.
Diabetes follow-up
- PPP goal: 80% of those estimated to have diabetes to have had a diabetes review.
What can your practice do?
Know how to identify and contact the high needs population in your practice:
- Use your practice management system to identify and flag Māori and Pacific peoples and people living in lower
socioeconomic areas
- Send invitations encouraging these patients to receive targeted services (e.g., influenza vaccinations, cervical screening)
- Ask these patients about their screening and immunisation status and record it in their notes in a way that is accessible
or searchable
Reflect on barriers that may prevent people in high needs populations from accessing services. Strategies to overcome
some of the common barriers include:
- Encourage all practice staff to have an understanding of barriers that may exist and be aware of strategies to overcome
these barriers
- Actively assist these patients to enrol in national screening programmes and make an appointment for them where necessary
- Ensure these patients know the cost of services and that some services, e.g. breast screening, are free
- Provide appropriate information about services
- Allow enough time to talk through any concerns
- Support patients who are shy or apprehensive
- Ensure patients know they can bring a support person
References
- District Health Boards New Zealand. PHO Performance Programme. Available from:
www.dhbnz.org.nz/Site/SIG/pho/PHO/About-the-Programme.aspx (Accessed
April, 2010).
- District Health Boards New Zealand. PHO Performance Programme Annual Report 1 July 2008 – 30 June 2009. Available
from:
www.dhbnz.org.nz/Site/SIG/pho/PHO/Annual-Reports.aspx (Accessed
April, 2010).
- Ministry of Health. PHO League table. 2009. Released under the official information act. Electronic copy available
from:
www.nzdoctor.co.nz (Accessed April, 2010).
- Ministry of Health. Tatau Kahukura: Māori health chart book, Public Health Intelligence monitoring report No.5.
Wellington; 2006.