Published: 13th March, 2026
Key practice points
- Symptoms of a UTI in young, pre-verbal children are often non-specific, e.g. fever, irritability, poor feeding and vomiting. Older children may be more able to describe lower urinary tract symptoms, e.g. painful or frequent urination, discoloured or malodorous urine, abdominal or back pain.
- A child’s risk of complications increases if UTI treatment is delayed, e.g. dehydration, febrile seizures, urosepsis
- Renal scarring can be a long-term complication of UTIs in children; risk is higher with an upper UTI, recurrent UTIs and in children with other complicating factors, e.g. genitourinary abnormalities
- Children with a suspected upper UTI generally require paediatric advice
- Children aged under three months and those of any age with symptoms or signs of significant systemic illness or complicating factors generally require referral for acute paediatric assessment
- Request laboratory urinalysis for all children with a suspected UTI, where possible; a mid-stream or clean catch urine sample is preferred
- Urine dipstick testing can support a suspected UTI diagnosis in a child with relevant symptoms and signs, but urine microscopy, culture and sensitivity analysis is required to confirm the diagnosis and microbial sensitivity
- Start empiric antibiotic treatment while awaiting laboratory urinalysis results. Treatment with oral cefalexin or nitrofurantoin for three days is recommended for children with mild, uncomplicated lower UTIs.
- Escherichia coli (E. coli) is the most common cause of UTIs in children
- Review empiric antibiotic choice once culture and sensitivity results are available, and select an alternative if the bacteria are resistant or the child’s symptoms have not improved
- Seek paediatric advice if the child does not respond to appropriate antibiotic treatment within 48 hours
- Imaging to identify potential genitourinary abnormalities is indicated for some children post-UTI. Refer all children aged under 12 months with their first UTI, and children of any age with an atypical or recurrent UTI, for a renal ultrasound, ideally to be conducted six weeks after presentation.
- Atypical UTIs include those that respond poorly to antibiotics within 48 hours, are caused by infection with a non-E. coli organism or are associated with known or suspected structural abnormalities or co-morbidities
- Recurrent UTI is defined as ≥ 2 proven episodes within one year, or ≥ 3 if symptoms were only mild
- Discuss strategies to help reduce the risk of future UTIs with parents/caregivers and children if age-appropriate, e.g. sufficient fluid intake, management of constipation, correct toileting technique
- Prophylactic antibiotic treatment is generally only indicated for children with known genitourinary abnormalities and will usually be initiated by a paediatric specialist
This is a revision of a previously published article. What’s changed:
- General article revision, including update of evidence and references
- Update of renal ultrasound referral recommendations consistent with the National Community Referral Criteria for Imaging (Phase 1), released September, 2025
- Updated antibiotic recommendations
- Inclusion of evidence on non-antibiotic prophylactic options for UTI prevention
Urinary tract infections (UTIs) affect approximately 5% of children, with incidence varying with age, sex and circumcision status.1, 2 The incidence of UTIs in children aged under 12 months is similar among females and uncircumcised males (~4%, risk is lower for circumcised males).2, 3 In children aged over 12 months, UTIs primarily affect females; female children aged 1 – 6 years are almost six times more likely to develop a UTI than males (cumulative incidence ~11% versus ~2%).3
Toilet training is often a time when children develop UTIs, as they learn bladder control and toileting hygiene.2 Other common causes of UTI include insufficient fluid intake, infrequent voiding or constipation.4 A UTI may also be the first indication of a previously unidentified genitourinary abnormality, e.g. in an infant.2 In older children, particularly females, a UTI may be associated with the early onset of sexual behaviour.2 A UTI is rarely a sign of sexual abuse, but this possibility should be considered if other risk factors are present.
For further information on when to consider abuse in children, see: https://www.nice.org.uk/guidance/cg89
E. coli is the most common cause of UTIs in children
Infection with Escherichia coli (E. coli) accounts for approximately 85 – 90% of UTIs in children.5 Other commonly implicated bacteria include Klebsiella, Proteus, Enterococcus and Enterobacter species.5 UTIs can be localised to the bladder (lower UTI; cystitis) or extend into the upper urinary tract and involve the kidneys (upper UTI; pyelonephritis).2
Risk factors associated with UTIs in children
There are many modifiable and non-modifiable risk factors that predispose children to developing a UTI (Table 1).
Table 1. Risk factors for UTIs in children.
| Non-modifiable |
Modifiable |
- Age under 12 months1, 2
- Female sex1
- Anatomic abnormalities of the urinary tract or kidneys1
- Previous renal surgery/implants1
- History of UTIs6
|
- Constipation1
- Poor fluid intake4
- Infrequent voiding, e.g. due to urinary holding4
- Overweight or obesity4
See: “Drink plenty and don’t hold on” |
Timely treatment is essential for reducing the risk of UTI-associated complications
Acute complications of a UTI in a child can include dehydration and febrile seizures.5 An untreated UTI can also progress to urosepsis, a potentially life-threatening complication.7 The primary aim of treatment is to resolve the UTI before it progresses to systemic infection.8 Timely treatment also reduces a child’s risk of developing permanent renal damage, i.e. renal scarring, following a UTI, see: “Prevention of long-term UTI complications in children”.
Young, pre-verbal children with a UTI will often present with non-specific symptoms that can be challenging to differentiate from those associated with common viral illnesses,7 for example:1, 6
- Fever
- Irritability
- Poor feeding
- Vomiting
The relevance of non-specific symptoms and signs should be assessed in the context of the child’s risk factors for developing a UTI (see: “Risk factors associated with UTIs in children”).
Older children are more likely to be able to describe symptoms specific to the urinary tract, such as:1
- Frequent or painful urination
- Changes to the colour or smell of urine
- Abdominal or back pain
A return to incontinence or bed-wetting in a toilet-trained child may also be suggestive of a UTI.5
Physical examination can help to identify a UTI
Findings on examination that may indicate a UTI include:5, 6
- Suprapubic or flank tenderness
- Palpable bladder or stool in the bowel on abdominal examination
- Abdominal distension
- Dehydration
- Fever
Further physical examination may also help to rule out alternative causes of fever.6 External genital examination may be indicated if anatomic abnormalities are suspected, e.g. phimosis, or there is clinical suspicion of an alternative diagnosis, e.g. vulvovaginitis.2
Distinguishing upper UTIs in children
Children with an upper UTI (pyelonephritis) are at increased risk of complications, particularly if antibiotic treatment is delayed.2 Therefore, any child presenting with symptoms of a UTI accompanied by fever ≥ 38°C and/or loin or flank pain/tenderness should be discussed with a paediatrician for consideration of hospital care.9
Indications for acute paediatric referral
Not all children with a suspected UTI will be suitable for treatment in the community, as intravenous (IV) antibiotics may be indicated.1
 Red flags for acute paediatric referral of a child with a suspected UTI include:1, 9
Red flags for acute paediatric referral of a child with a suspected UTI include:1, 9
- Age under three months
- Symptoms or signs of significant systemic illness or sepsis
- The presence of complicating factors, e.g. an abdominal or bladder mass, impaired renal function, anatomic urinary tract abnormalities, previous renal surgery/implants
For further information on identifying the risk of serious illness in young children with fever, see: https://bpac.org.nz/2024/fever.aspx
Ideally, a urine sample will be collected from any child with a suspected UTI to either:1
- Confirm the diagnosis if symptoms and signs suggest a UTI, OR
- Rule out a UTI if symptoms and signs are uncertain, e.g. fever of unknown origin
Collect a urine sample before antibiotics are initiated where possible, see: “Collecting a urine sample from a child”.9 Initiate empiric antibiotic treatment on the basis of clinical suspicion in a child with clear symptoms and signs of a UTI while awaiting culture and sensitivity results; do not delay treatment if a urine sample cannot be obtained.9
Collecting a urine sample from a child
Obtaining a urine sample from a young child can be challenging and potential contamination associated with the method of collection must be considered.7 Clean catch is the preferred method for urine collection; mid-stream urine samples are associated with lower rates of contamination but may not be possible to obtain from all children.2, 9 Table 2 (below) provides an overview of urine collection methods that can be carried out in primary care.
Table 2. Methods of urine sample collection in children aged three months to 12 years in a primary care setting.1, 2
| Indication |
Method |
Procedure |
Contamination rate |
Children able to void on request |
Mid-stream urine (MSU) |
In uncircumcised males, retract the foreskin, if possible; in females, part the labia. Allow the child to urinate into the toilet and collect a mid-stream sample in a sterile container. Some children may be able to collect their own sample with supervision. |
~24% |
Children unable to void on request |
Clean catch (CCU) |
Clean the genital area for 10 seconds with chlorhexidine solution and gauze; dry with a sterile swab. Collect a urine sample in a sterile container when the child voids spontaneously, ideally from mid-stream.
The quick wee method may be used to induce urination in infants aged 3 – 12 months: use gauze soaked in cold saline to rub the suprapubic area in a circular motion. |
~26% |
Urine bag
N.B. Urine bag samples are only suitable for dipstick testing; a MSU or CCU sample is required for microscopy, culture and sensitivity analysis. |
Clean and dry the genital area as above. Attach an adhesive urine bag and apply a nappy on top, as normal. Check the bag at regular intervals and collect the urine sample in a sterile container as soon after voiding as possible. Replace with a new bag after four hours if a sample has not been obtained. |
50 – 60% |
Best Practice Tip: If a urine sample cannot be obtained in the clinic, parents/caregivers may be able to collect a sample at home; ideally, within 24 hours.9 Provide clear instructions and all necessary supplies, including chlorhexidine solution and sterile gauze swabs if genital area cleaning is required, and advise them to return the sample as soon after collection as possible. Perform dipstick testing before sending the sample for laboratory urinalysis, if practical (see: “The role of dipstick urinalysis”).
The role of dipstick urinalysis
Urine dipstick testing for leukocyte esterase and nitrite can be used as an initial indication of a UTI diagnosis in children aged over three months.1, 9 However, urine microscopy, culture and sensitivity analysis is still required to confirm a presumptive diagnosis and antibiotic sensitivity.1
Perform dipstick urinalysis on fresh urine.1 If the sample was collected by a parent/caregiver, ensure it is tested within one hour of collection if stored at room temperature, or within four hours if refrigerated.1
Interpreting urine dipstick results in children
The presence of leukocyte esterase alone does not confirm a UTI, as pyuria can occur with other infections.7 Similarly, the absence of nitrite does not exclude a UTI, as some species of uropathogenic bacteria, e.g. Enterococcus, do not metabolise nitrate.10 Nitrite production also takes approximately four hours; results can therefore be less reliable in children who void frequently, e.g. infants.10
The interpretation of urine dipstick test results in children differs by age:
In children aged three months to three years, a positive dipstick test result for either leukocyte esterase or nitrite is sufficient to initiate empiric antibiotic treatment and send the urine sample for microscopy, culture and sensitivity analysis.9
N.B. Urine dipstick testing is not recommended in children aged under three months as the results are unlikely to impact clinical decision making; if a UTI is suspected, referral for acute paediatric assessment is indicated.1
In children aged 3 – 12 years, a presumptive UTI diagnosis can be made based on a positive dipstick test result for both leukocyte esterase and nitrite (Figure 1); initiate empiric antibiotics and send the urine sample for microscopy, culture and sensitivity analysis.1 A positive result for either leukocyte esterase or nitrite is usually sufficient to proceed with empiric antibiotic treatment if characteristic UTI symptoms and signs are present (Figure 1); send the urine sample for microscopy, culture and sensitivity analysis.1
In all children aged over three months, a negative dipstick test result for both leukocyte esterase and nitrite suggests that a UTI is unlikely and that a urine sample should not be sent for laboratory urinalysis; consider alternative diagnoses.1 However, if clinical suspicion persists, e.g. there is concern about the reliability of the dipstick test, include relevant clinical information on the form sent with the sample to the laboratory.9 N.B. A urine sample that is negative for pyuria on microscopy is unlikely to be cultured.
Urine bag samples can be used for dipstick testing but are inappropriate for laboratory urinalysis due to high rates of contamination; a mid-stream or clean catch urine sample should ideally be obtained, see: “Collecting a urine sample from a child”.1
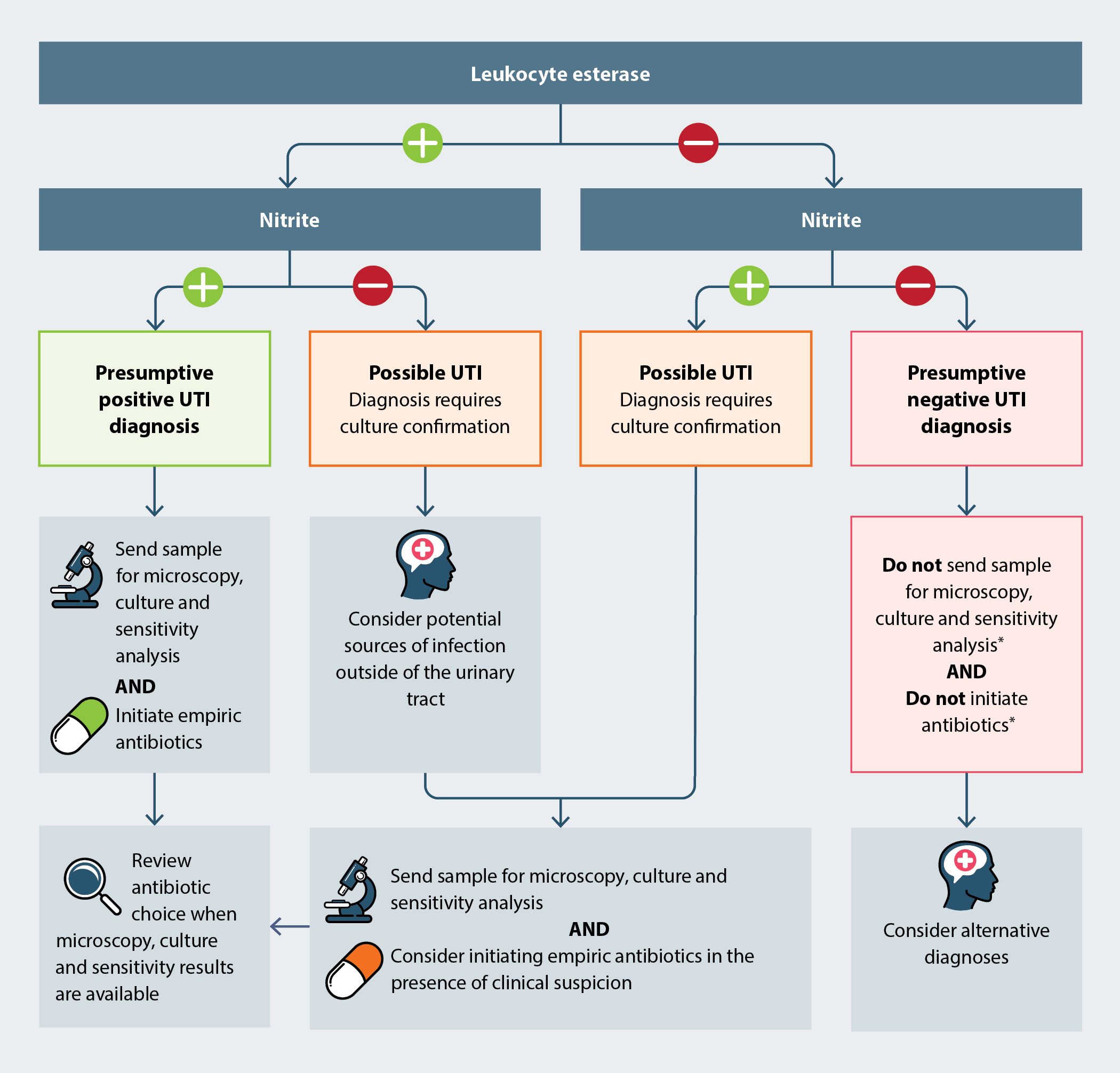
Figure 1. Interpreting dipstick test results for urine samples obtained from children aged 3 – 12 years.1, 9
* Use clinical judgment; if dipstick results do not correlate with the child’s symptoms and signs and clinical suspicion of a UTI persists, laboratory urinalysis may be appropriate
For further information on the interpretation of urine dipstick and microscopy, culture and sensitivity results in children, see: https://www.starship.org.nz/guidelines/urinary-tract-infection/
Children aged over three months with a lower UTI can generally be managed in primary care with oral antibiotics, unless their symptoms or signs are severe or they have complicating factors (see: “Indications for acute paediatric referral”). Empiric treatment can be initiated with clinical evidence of a UTI, with antibiotic choice reviewed once urine microscopy, culture and sensitivity results are available.
Selecting an oral antibiotic
Cefalexin is the preferred first-line antibiotic option for empiric treatment of mild lower UTIs in children, followed by nitrofurantoin.1 When sensitivity results are available, other antibiotics, such as amoxicillin + clavulanic acid or trimethoprim + sulfamethoxazole may be appropriate, depending on local resistance data (see: “Review antibiotic choice once urine culture and sensitivity results are available”).1 See Table 3 (below) for dosing information.
Table 3. Oral antibiotics for mild lower UTIs in children aged three months to 12 years.1, 8, 11 For information on contraindications, monitoring, adverse effects and interactions, refer to the New Zealand Formulary for Children (NZFC): https://www.nzfchildren.org.nz/nzf_1.
| Order of preference |
Empiric treatment |
 |
Cefalexin |
25 mg/kg/dose, three times daily (maximum 500 mg/dose), for three days |
Nitrofurantoin* (immediate-release) |
1.5 mg/kg/dose, four times daily (maximum 50 mg/dose), for three days
N.B. There is no funded liquid formulation of nitrofurantoin available. However, immediate-release tablets can be can be compounded into a 10 mg/mL suspension (funded if the child is unable to swallow tablets). |
If bacteria are known to be sensitive |
Amoxicillin + clavulanic acid |
30 mg/kg/dose, three times daily (maximum 625 mg/dose), for three days |
Trimethoprim + sulfamethoxazole |
24 mg/kg/dose, twice daily (maximum 960 mg/dose), for three days |
|
A longer course, e.g. up to seven days, may be considered in children with more severe symptoms but no red flags for secondary care referral |
* Avoid in children with renal impairment or if an upper UTI is suspected (paediatric advice is usually indicated)
N.B. Antibiotic choice may be influenced by local resistance data. If in doubt regarding antibiotic selection, seek local microbiology advice.
A three-day course of antibiotics is recommended for both male and female children with mild, uncomplicated lower UTIs in the community.8 Current evidence suggests that short courses (2 – 4 days) of antibiotics are equally as effective as longer courses (7 – 14 days) for the treatment of lower UTIs in children without fever, with no increase in recurrence.12 A longer course, e.g. up to seven days, may be considered in children with more severe symptoms but no red flags for secondary care referral (see: “Indications for acute paediatric referral”).1
Provide advice to parents/caregivers about supportive care measures, including ensuring the child remains well hydrated and the use of paracetamol and/or ibuprofen for pain relief, as required.8
Review antibiotic choice once urine culture and sensitivity results are available
If the child’s urine culture and sensitivity results report resistance to the empiric antibiotic that was prescribed and their symptoms are not improving, select an alternative (Table 3); prescribe a narrow-spectrum antibiotic wherever possible.13
Ideally, all children receiving empiric antibiotic treatment for a UTI should be reviewed within 48 – 72 hours.1 However, this may not always be feasible; advise parents/caregivers to bring the child back for reassessment if their symptoms worsen or do not improve within 48 hours, or schedule a follow-up phone call appointment.
Consider seeking paediatric advice for children with a UTI whose symptoms do not respond to suitable antibiotic treatment within 48 hours.9
Approximately 30% of children with a UTI will be diagnosed with another within six to 12 months.14 Recurrence can occur as a result of either:15
- Relapse – further infection with the same organism
- Re-infection – subsequent infection with a new organism
UTIs are considered recurrent when a child experiences ≥ 2 culture-proven UTIs within one year, or ≥ 3 if the symptoms were only mild.1
Treatment of a recurrent UTI is consistent with acute UTIs (see: “Treatment of UTIs in children”). Consider previous urine culture and sensitivity results and the potential for resistance associated with previous antibiotic use when deciding on empiric treatment.13 Also see: “When is a renal ultrasound indicated?”
Routine antibiotic prophylaxis for recurrent UTIs in children is not recommended, as the benefit is modest and there is an increased likelihood of microbial resistance.15, 17 A 2019 Cochrane review reported that low-dose antibiotic prophylaxis over 12 months reduced the estimated absolute risk of repeat symptomatic UTIs by 6% in children with or without vesicoureteral reflux (VUR; the backflow of urine from the bladder to the ureters or kidneys)18 and was associated with a two-fold increase in microbial resistance.17 Antibiotic prophylaxis for recurrent UTI is generally only indicated in children with known genitourinary abnormalities, and is usually initiated by a paediatric specialist.8, 19
A breakthrough UTI is an infection that occurs while a child is taking antibiotic prophylaxis.2 This can occur due to infection with bacteria resistant to the prophylactic antibiotic, non-adherence to the antibiotic regimen or significant genitourinary abnormalities.2 When treating a child with a breakthrough UTI, prescribe a different antibiotic to the one being taken for prophylaxis.19
An estimated 3 – 15% of children develop permanent renal damage, i.e. renal scarring, following their first UTI.14 A child’s risk of renal scarring increases with subsequent UTIs; a 2019 study of children without known genitourinary abnormalities in the United States reported an incidence of renal scarring post-initial febrile UTI of approximately 2.8% (95% confidence interval [CI]: 1.2 – 5.8%), increasing to approximately 25.7% after two (95% CI: 12.5 – 43.3) and 28.6% (95% CI: 8.4 – 58.1) after three.5, 20 Other risk factors for renal scarring include genitourinary abnormalities, e.g. high-grade vesicoureteral reflux, infection with a non-E. coli organism and delayed initiation of treatment.5
Cumulative renal scarring as a result of recurrent UTIs can impair renal function, resulting in chronic renal failure.2 The early identification of risk factors for renal scarring and UTI recurrence is, therefore, essential for reducing a child’s risk of long-term complications.
When is a renal ultrasound indicated?
The primary role of a renal ultrasound in a child following a lower UTI treated in the community is to identify genitourinary abnormalities that may predispose them to recurrent UTIs, increase their risk of renal scarring and/or require long-term management.7, 21
A request for a renal ultrasound, ideally to be performed six weeks after presentation, is indicated in:16
- Children aged < 12 months with their first UTI
- Children of any age with an atypical UTI who have not previously been investigated with a renal ultrasound*, defined as:
- Poor response to antibiotics after 48 hours
- Poor urine flow/suspected urinary obstruction
- Abdominal or bladder mass
- Raised creatinine
- Hypertension
- Infection with a non-E. coli organism
- Children of any age with recurrent UTI (see: “Recurrent UTIs in children”) who have not previously been investigated with a renal ultrasound*
* A repeat renal ultrasound may be indicated if a child re-presents with an atypical or recurrent UTI > 12 months after their previous renal ultrasound; seek paediatric advice16
As a child’s risk of developing renal scarring increases with subsequent UTIs, prevention of recurrence is a key aspect of UTI management in children.2
“Drink plenty and don’t hold on”
Educate parents/caregivers, and children, if age appropriate, about measures to prevent UTI recurrence. Constipation and poor fluid intake are significant contributing factors to the development of UTIs in children.1, 4 Parents/caregivers should be advised to ensure that their child drinks sufficient fluids daily in frequent, small amounts, and that their dietary fibre intake is adequate to prevent or alleviate constipation.9 If constipation is significant or persistent, pharmacological management may be considered, e.g. lactulose.8
Reinforce teaching correct toileting technique to children out of nappies, e.g. wiping from front to back for females, encouraging the child not to “hold on” and go to the toilet as needed.9
Children with refractory or severe voiding dysfunction require referral to secondary care as they have an increased risk of recurrent UTI. Return to normal voiding is vital to reduce this risk.
There is little evidence associating scented bath products with UTIs in children
In some children, the use of scented bath products, such as soaps, gels and bubble baths, can cause genital irritation and discomfort and induce lower urinary symptoms that are often associated with a UTI, e.g. dysuria.5, 22 However, there is little evidence suggesting that these products increase a child’s risk of developing a UTI or that avoidance reduces their risk.5, 23
Children who experience genital irritation and those with recurrent UTI may benefit from limiting their exposure to scented bath products; consider a mild, soap-free cleanser, e.g. aqueous cream, as an alternative. Educate parents about correct genital cleaning techniques, if appropriate (see: “Resources for parents and caregivers”).
The evidence supporting the use of non-antibiotic prophylactics for UTI prevention in children is limited
Various non-antibiotic treatments have been investigated for UTI prophylaxis in children, including:
 Cranberry products. Should generally only be considered for UTI prophylaxis in children after seeking paediatric advice.19 A 2023 Cochrane review found that the use of cranberry products was associated with a reduction in the risk of repeat symptomatic UTI in children without neurogenic bladders (risk ratio [RR]: 0.46, 95% CI: 0.32 – 0.68; five studies, N = 504); four studies used cranberry juice and one used cranberry tablets.24 These findings provide moderate evidence supporting the efficacy of cranberry products for UTI prevention in children.24 However, cranberry juice is high in sugar, and commercial formulations in capsules or tablets may not be suitable for younger children. Ensure that parents/caregivers understand that cranberry products are not suitable for the treatment of a UTI and that they need to seek medical attention if the child develops UTI symptoms.9
Cranberry products. Should generally only be considered for UTI prophylaxis in children after seeking paediatric advice.19 A 2023 Cochrane review found that the use of cranberry products was associated with a reduction in the risk of repeat symptomatic UTI in children without neurogenic bladders (risk ratio [RR]: 0.46, 95% CI: 0.32 – 0.68; five studies, N = 504); four studies used cranberry juice and one used cranberry tablets.24 These findings provide moderate evidence supporting the efficacy of cranberry products for UTI prevention in children.24 However, cranberry juice is high in sugar, and commercial formulations in capsules or tablets may not be suitable for younger children. Ensure that parents/caregivers understand that cranberry products are not suitable for the treatment of a UTI and that they need to seek medical attention if the child develops UTI symptoms.9
 Probiotics. There is currently insufficient evidence supporting the efficacy of probiotics for UTI prophylaxis in children; European Association of Urology (EAU) paediatric guidelines recommend that they are only considered as an adjuvant in children prescribed antibiotic prophylaxis (see: “Recurrent UTIs in children”).2, 19 The limited available evidence regarding the efficacy of probiotics for preventing UTI recurrence in children is conflicting.2 However, the results of a 2021 meta-analysis and systematic review suggest that they may provide some benefit; in children without genitourinary abnormalities (two clinical trials, N = 234), probiotics containing Lactobacillus reduced the risk of UTI recurrence by ~50% relative to placebo (RR: 0.52, 95% CI: 0.29 – 0.94).25 In children with primary vesicoureteral reflux (two clinical trials, N = 248), no difference in risk of recurrence was observed with Lactobacillus probiotics relative to antibiotic prophylaxis (RR: 0.82, 95% CI: 0.56 – 1.21) but the risk of antimicrobial resistance was significantly lower (RR: 0.38, 95% CI: 0.21 – 0.69).25 This analysis only included a small number of clinical trials using different probiotic products; further investigation in larger trials is required to confirm probiotic efficacy and determine the optimal strain and dosing regimen.
Probiotics. There is currently insufficient evidence supporting the efficacy of probiotics for UTI prophylaxis in children; European Association of Urology (EAU) paediatric guidelines recommend that they are only considered as an adjuvant in children prescribed antibiotic prophylaxis (see: “Recurrent UTIs in children”).2, 19 The limited available evidence regarding the efficacy of probiotics for preventing UTI recurrence in children is conflicting.2 However, the results of a 2021 meta-analysis and systematic review suggest that they may provide some benefit; in children without genitourinary abnormalities (two clinical trials, N = 234), probiotics containing Lactobacillus reduced the risk of UTI recurrence by ~50% relative to placebo (RR: 0.52, 95% CI: 0.29 – 0.94).25 In children with primary vesicoureteral reflux (two clinical trials, N = 248), no difference in risk of recurrence was observed with Lactobacillus probiotics relative to antibiotic prophylaxis (RR: 0.82, 95% CI: 0.56 – 1.21) but the risk of antimicrobial resistance was significantly lower (RR: 0.38, 95% CI: 0.21 – 0.69).25 This analysis only included a small number of clinical trials using different probiotic products; further investigation in larger trials is required to confirm probiotic efficacy and determine the optimal strain and dosing regimen.
 Methenamine hippurate. This medicine is not recommended for use in children aged under 12 years in New Zealand.8 However, National Institute for Health and Care Excellence (NICE) guidelines from the United Kingdom recommend that methenamine hippurate may be considered as an alternative to daily antibiotic prophylaxis in children aged over six years with recurrent UTI under specialist advice.9
Methenamine hippurate. This medicine is not recommended for use in children aged under 12 years in New Zealand.8 However, National Institute for Health and Care Excellence (NICE) guidelines from the United Kingdom recommend that methenamine hippurate may be considered as an alternative to daily antibiotic prophylaxis in children aged over six years with recurrent UTI under specialist advice.9
 D-mannose. There is currently insufficient evidence supporting the use of D-mannose for UTI prophylaxis in children.19 A 2022 Cochrane review did not identify any randomised controlled trials investigating the efficacy of D-mannose for the prevention or treatment of UTIs in children.26
D-mannose. There is currently insufficient evidence supporting the use of D-mannose for UTI prophylaxis in children.19 A 2022 Cochrane review did not identify any randomised controlled trials investigating the efficacy of D-mannose for the prevention or treatment of UTIs in children.26
Resources for parents and caregivers





