Published: 27th March, 2026
Key practice points
- Chronic kidney disease (CKD) is broadly defined as any abnormality of kidney function or structure over a period longer than three months with implications for the patient’s health. It is associated with a substantial increase in cardiovascular disease (CVD) risk, particularly as kidney function declines further.
- The damage associated with CKD is generally not reversible, but progression can be slowed and the risk of CVD reduced with appropriate management of the underlying cause and modifiable risk factors
- Patients often experience a marked reduction in kidney function before symptoms become apparent. Therefore, testing for CKD every one to two years is recommended based on the presence of risk factors, e.g. diabetes, hypertension, Māori/Pacific or South-Indo Asian ethnicity, increasing age.
- Measure blood pressure and check serum creatinine to estimate glomerular filtration rate (eGFR) and urine albumin:creatinine ratio (ACR)
- If eGFR or urine ACR results are abnormal (i.e. eGFR < 60 mL/min/1.73 m2 or urine ACR ≥ 3 mg/mmol), repeat testing over the next three months depending on the clinical situation to confirm CKD
- CKD is classified according to the patient’s eGFR category (G1 – G5), degree of persistent albuminuria (A1 – A3) and the underlying cause (if identified); this classification informs management decisions
- Management of patients with CKD is achieved through lifestyle changes (e.g. weight loss, exercise, reducing sodium intake) and pharmacological treatment targeting albuminuria, hypertension and hyperglycaemia or any other underlying cause
- A low-protein diet is not necessary in most cases, and should only be undertaken with guidance from a nephrologist or dietitian
- Combination pharmacological treatment (termed the “four pillars” approach) is becoming the new standard of care for patients with CKD, particularly for those with diabetes and at high risk of progression. Depending on patient co-morbidities, this may include:
- An ACE inhibitor or ARB; and
- A SGLT-2 inhibitor; and/or
- A GLP-1 receptor agonist; and/or
- A non-steroidal mineralocorticoid receptor antagonist
In New Zealand, medicines availability (non-steroidal MRAs) and Special Authority funding restrictions (SGLT-2 inhibitors and GLP-1 receptor agonists) will influence the ability to adopt the “four pillars” approach for patients with CKD, however, use of these medicines should be prioritised wherever possible.
- Regular ongoing monitoring is important to assess treatment efficacy, detect progressive kidney function decline and to identify indications for referral to a nephrologist
- Ensure patients have a “sick day” plan, i.e. they know which medicines to temporarily avoid if they develop an acute illness
This is a revision of a previously published article. What’s new for this update:
- Full article revision and update of evidence
- Section added on the causes of CKD and inclusion of information on vaccination recommendations
- Focus on the “four pillars” approach to the management of CKD
- Revised metformin dosing in renal impairment
Chronic kidney disease (CKD) is the term broadly used to describe persistent abnormalities in kidney structure or function.1 However, declining kidney function is also a natural part of the ageing process.1, 2 It is estimated that by age 70 years, approximately 30% of the population will meet classification criteria for CKD.2, 3
There is considerable interconnectedness between the cardiovascular system, kidneys and metabolic risk factors (e.g. diabetes, obesity). The term "cardiovascular-kidney-metabolic (CKM) syndrome” is being increasingly used in the literature. CKM syndrome describes a systemic disorder defined by pathophysiological interactions among these three factors, resulting in multi-organ dysfunction/damage and adverse CVD outcomes.4, 5 For example, damaged kidneys are less able to control blood pressure and regulate blood glucose levels. Diabetes and hypertension are the most frequent underlying causes of CKD (see Figure 1 for a list of risk factors).6, 7 CKD is associated with a substantially increased risk of cardiovascular disease (CVD), morbidity and mortality.1, 3 CKD rarely occurs in isolation, therefore, a “whole system” approach to management is required to improve patient outcomes.
While CKD itself is generally not reversible, cardio-renal-metabolic risk and progression to advanced CKD and end-stage kidney failure requiring dialysis or renal transplant can be reduced through early identification and management of the underlying cause of CKD and associated risk factors/co-morbidities.
New national guidance on optimising cardiovascular-kidney-metabolic health is being developed by cardiac, renal, diabetes and stroke national clinical networks in conjunction with Te Whatu Ora; a link to the published guidance will be added once it is available.
CKD in New Zealand
CKD affects approximately one in ten people globally.1, 7 Prevalence is expected to continue to rise with an ageing population and higher incidence of co-morbidities, e.g. diabetes and hypertension.7, 8 While there are no overall prevalence data for CKD in New Zealand, regional estimates are consistent with global figures; an Auckland-based study involving the analysis of health records of over 25,000 patients in 2015 – 2017 reported a CKD prevalence of 13%.9 However, there was significant variation in prevalence by ethnicity, e.g. 17.8% for Samoan and 10.4% for Māori compared to 7.1% for non-Pacific/non-Māori.9 An analysis of electronic health records of over 200,000 patients in the Otago-Southland region in 2014 estimated the prevalence of CKD to be 11.8%.10
The impact of CKD on communities in New Zealand is increasing and the number of people requiring dialysis has more than doubled over the last 20 years.3, 11 As of 2024, a total of 3,314 people were reportedly undergoing dialysis in New Zealand, and 2,433 people were living with a kidney transplant.11 Kidney failure is more prevalent among people of Māori/Pacific ethnicity (see: “Ethnic inequities in CKD”). Diabetes is usually the most common primary cause of CKD in people with kidney failure.11
Ethnic inequities in CKD
CKD disproportionately affects certain ethnic groups, e.g. Māori, Pacific and South/Indo Asian peoples, which is likely in part due to the higher prevalence of risk factors for CKD (e.g. diabetes and hypertension) in these populations, as well as barriers to accessing healthcare.3, 8
Clinical practice guidelines for CKD in Māori have been developed (2023), along with recommendations for health systems and providers to prioritise actions to achieve equitable outcomes in kidney health for Māori.12 These recommendations are also likely to be relevant to Pacific and South/Indo Asian peoples who, like Māori, experience a higher burden of CKD/CVD. A key point emphasised in the guidelines is early CVD risk assessment, including urine albumin:creatinine ratio (ACR)/serum creatinine to detect CKD as soon as possible (see: “Screening for kidney risk in Māori”).12
A range of system-level changes are proposed to improve CKD outcomes for Māori, including better data collection, more effective and linked information/referral systems, as well as addressing the social determinants driving inequitable kidney health outcomes, e.g. poverty, housing.12 At the clinician-level, outcomes can be improved by completing cultural safety training, and utilising an Indigenous Health Framework to guide the care narrative. For Māori patients, this may include:12
- Enhancing engagement during appointments through respect, reciprocation and use of Māori customs, e.g. mihimihi (initial greeting engagement), whakawhanaungatanga (making a connection), kaupapa (addressing the purpose of the encounter) and poroporoaki (closing the session)
- Considering all aspects of hauora (health and wellbeing): taha tinana (physical), taha hinengaro (mental), taha whānau (family and social) and taha wairua (spiritual). This outlook can help identify additional perspectives, issues and concerns that may influence the success of management decisions.
- Pacific frameworks for health and wellbeing include the Fonofale (Pan-Pacific & Samoan) and Fonua models (Tongan)
- Including whānau/family where possible when conveying information around CKD, discussing management and establishing goals of care
CKD is defined as abnormalities of kidney structure or function, present for at least three months, with implications for health.1 Specifically:1, 13
- An estimated or measured GFR of < 60 mL/min/1.73 m2 with or without evidence of kidney damage; OR
- Evidence of kidney damage with or without reduced eGFR, including one or more of the following:
- Albuminuria, i.e. urine ACR ≥ 3 mg/mmol (most common marker of kidney damage)
- Haematuria after exclusion of urological causes
- Urine microscopy abnormalities, e.g. casts
- Electrolyte or other abnormalities due to tubular disorders, e.g. renal tubular acidosis, nephrogenic diabetes insipidus, renal potassium wasting
- Abnormalities detected by histology, e.g. glomerular disease
- Structural abnormalities detected by imaging, e.g. polycystic or dysplastic kidneys, renal artery stenosis
Classifying CKD
The Kidney Disease: Improving Global Outcomes (KDIGO) criteria (Table 1) are used to classify patients with CKD according to their eGFR category (G1 – G5), degree of persistent albuminuria (A1 – A3) and the underlying cause (see: “Diabetes and hypertension are the most common causes of CKD”).1 This is referred to as the Cause, Glomerular filtration rate and Albuminuria (CGA) classification system. For example, a patient’s CKD classification may be: CKD G3a with microalbuminuria (A2) due to diabetes. The eGFR and persistent albuminuria categorisation can provide predictive information on prognosis and help guide decisions around monitoring and treatment.
Table 1. Categorisation and prognosis of CKD according to GFR and persistent albuminuria categories.* Adapted from KDIGO, 2024.1
* Prognostic risk broadly relates to “CKD outcomes” which includes various factors such as progression to kidney failure, complications, e.g. acute kidney injury, CVD, morbidity and mortality.1,14 This information is intended to help clinicians triage patients with CKD and inform the intensity of management and monitoring required, as well as the need for nephrologist referral (see: Figure 1 and “Patients requiring nephrologist referral” for further information). N.B. The specific risk percentage associated with individual outcomes is not given within general risk categories.
Diabetes and hypertension are the most common causes of CKD
Diabetes and hypertension are the predominant causes of CKD.6, 7 Other causes include tubulointerstitial disease, systemic disease affecting the kidney (e.g. autoimmune disorder), glomerular disease (e.g. glomerulonephritis, nephrotic syndrome), renal vascular disease, urinary obstruction or familial/hereditary kidney disease.6, 8 The cause of a patient’s CKD will usually either be evident when considering their history/co-morbidities, or determined during the diagnostic work-up following abnormal laboratory findings (see: “Identify the underlying cause of CKD: other tests to request”).6, 7
Distinguishing progressive CKD from age-related kidney function decline
Gradual decline in kidney function is considered a normal part of the ageing process, and age is a variable in the formula for calculating eGFR.1, 2 In the general population, eGFR declines by approximately 1 mL/min/year, and many older patients will meet criteria for CKD G3a (Table 1) without having any evidence of structural kidney disease.3 There is some discussion in the literature regarding the establishment of age-adapted CKD classifications but as yet, no consensus has been reached.15
A clinical consideration when interpreting eGFR results is to differentiate patients with progressively deteriorating kidney function due to disease from those with uncomplicated, age-related kidney function decline. A sustained decrease in eGFR of 10 – 15 mL/min/1.73 m2 or ≥ 25% reduction and a change in eGFR category within 12 months usually indicates progressive CKD;7, 13 patients who meet these criteria usually require discussion with, or referral to, a nephrologist.
CKD is associated with increased CVD risk
Reduced eGFR and albuminuria are independent risk factors for CVD.13 Even in the early stages, CKD is a significant risk factor for CVD events and mortality, and this risk increases further as kidney function declines.1, 16 People with CKD are up to 20-times more likely to die from a cardiovascular event than require a kidney transplant or dialysis.13
The association between CKD and CVD exists in part because two of the largest risk factors for CKD – diabetes and hypertension – are also associated with left ventricular hypertrophy and other changes to the heart and vasculature which can result in major adverse cardiovascular outcomes, e.g. myocardial infarction, stroke.16 Other suggested mechanisms include vascular calcification, dyslipidaemia, inflammation and endothelial dysfunction.16 People with CKD often have characteristic changes in the myocardium, including collagen deposition and fibrosis, and cardiac hypertrophy.16 Early detection of CKD in groups with an already high CVD risk, e.g. Māori and Pacific peoples, should therefore be a priority (see: “Screening for kidney risk in Māori”).
People with CKD are generally asymptomatic in the early stages and in some cases, kidney function can reduce by up to 90% before symptoms develop.13 If symptoms are present, they are often non-specific, e.g. nocturia, malaise, anorexia, nausea, pruritus, restless legs, dyspnoea, oedema, cognitive impairment.13 Therefore, to increase the detection of CKD in primary care, a risk-based approach to investigation is recommended (Figure 1).3, 13
To investigate for CKD, request:1, 3, 13
eGFR reported from New Zealand laboratories is usually calculated with the CKD-EPI algorithm as this is now the recommended equation and considered most accurate. N.B. The Cockcroft-Gault equation may be used to guide dose adjustments for certain medicines; a calculator is available from the NZF.
- Urine ACR, to determine albuminuria status. Ideally obtain a first void mid-stream urine sample but a random urine sample is acceptable. Albuminuria is one of the most important factors for determining CKD progression and CVD risk; persistently elevated levels may influence the decision to initiate or escalate treatment, even in patients with a more preserved eGFR.1, 17 N.B. Urine dipstick to check for proteinuria is generally not sufficient for the purpose of CKD testing.1, 13
Albumin:creatinine ratio is preferable to protein:creatinine ratio in most cases. ACR is considered to be a more sensitive and specific measure of changes in glomerular permeability.1, 18 Evaluation of protein:creatinine ratio may be appropriate when non-albumin proteinuria is suspected, e.g. disorders of tubular function, multiple myeloma.1, 6
A risk-based approach to detecting CKD
A kidney health check is recommended every one to two years for patients with risk factors for CKD (e.g. hypertension, diabetes, Māori, Pacific or South/Indo Asian ethnicity, increasing age; see Figure 1 for a list of risk factors):3, 13, 19
- Measure blood pressure
- Request serum creatinine (for eGFR)
- Obtain and send a sample for urine ACR
Patients with diabetes, hypertension or a history of acute kidney injury should undergo annual investigation for CKD, and be offered lifestyle advice to reduce their cardio-renal-metabolic risk (see: “Lifestyle management of CKD”).13
Population screening for CKD in isolation is not currently recommended.1, 3
Screening for kidney risk in Māori
Caring for Australians and New Zealanders with Kidney Impairment (CARI) guidelines recommend screening for kidney risk by calculating the five-year CVD risk using New Zealand Primary Prevention Equations for:12
- Māori males aged 30 years and over
- Māori females aged 40 years and over
- Māori with diabetes from diagnosis
In addition, it is noted that CVD risk assessment should include urine ACR and serum creatinine (for eGFR) testing for all Māori patients.12 N.B. These parameters are typically not included in general CVD risk calculators, but are often included in tools tailored for use in people with diabetes.
Recommendations around early CVD testing (including urine ACR and serum creatinine assessment) are also likely to apply to Pacific and South/Indo Asian peoples who, like Māori, experience a higher burden of CKD/CVD.
Cystatin C testing is not routinely required but may be useful in some scenarios
Creatinine-based estimation of GFR (eGFRcr) is generally sufficient for most patients when investigating for CKD.1, 7 An alternative method of estimating GFR from a combination of creatinine and cystatin C (eGFRcr-cys) is gaining traction in some overseas guidelines. Cystatin C testing is available and funded in New Zealand but is not recommended for routine use.
KDIGO guidelines recommend cystatin C testing if there is uncertainty around the accuracy of eGFR based solely on creatinine (i.e. over or underestimation) and if the eGFR will affect clinical decision making.1 An advantage of cystatin C testing is that its production rate is constant, and is less affected by factors such as age, sex, ethnicity or muscle mass than creatinine. Therefore, groups who might benefit from eGFRcr-cys include those with abnormally high or low muscle mass (e.g. people who are body builders, with an eating disorder or amputation), severe obesity or malnourishment.1 Another scenario where eGFRcr-cys could be useful is when a more accurate eGFR for medicine dosing is needed, e.g. when prescribing metformin it may be appropriate to determine the patient’s eGFR from both creatinine and cystatin C results if the creatinine-based eGFR result is in a borderline range, and it is therefore uncertain if a dose reduction is required.
Online calculators can be used to determine the patient’s eGFR from both creatinine and cystatin C results, e.g. https://www.kidney.org/professionals/gfr_calculator.
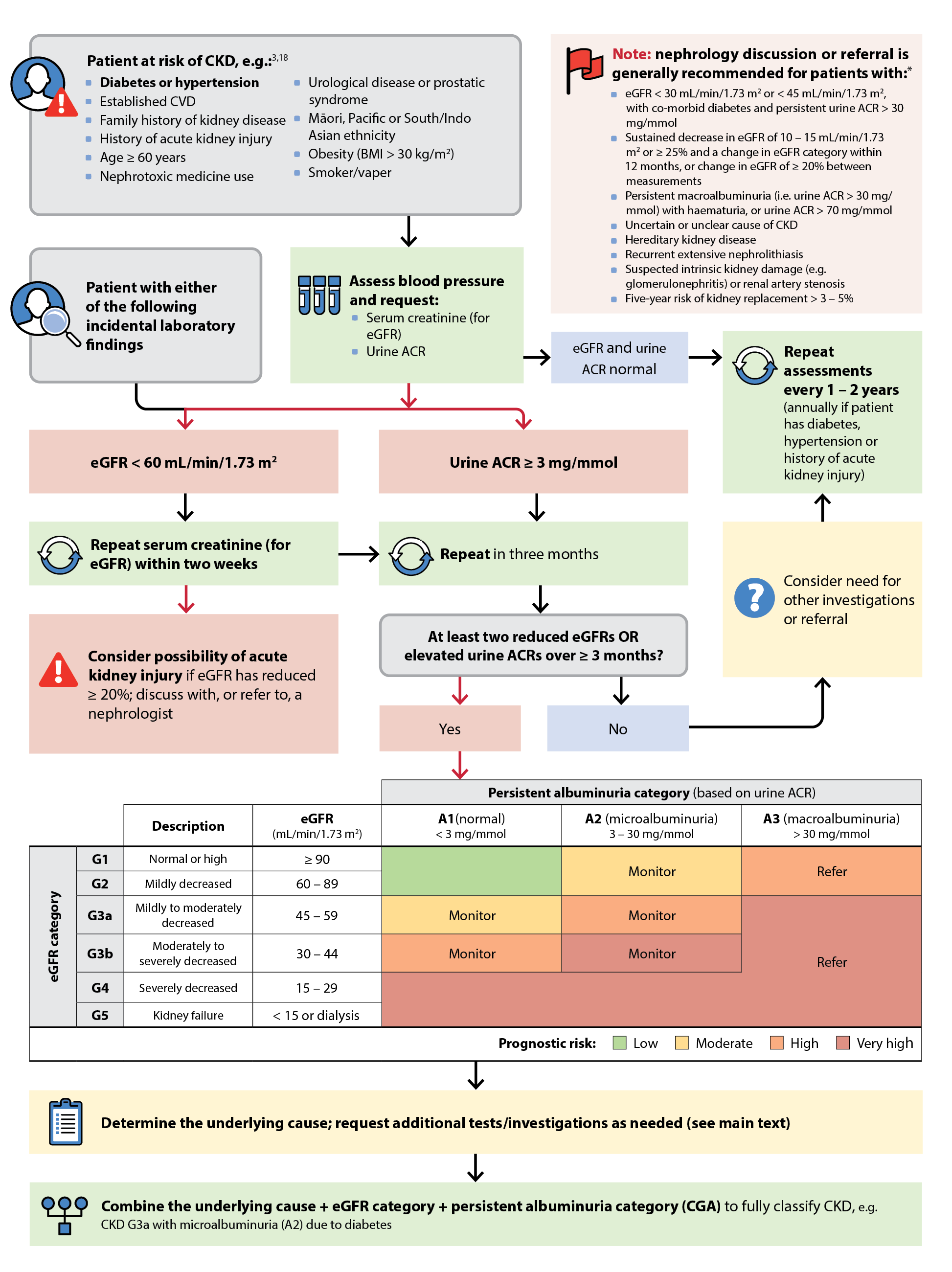
Figure 1. Algorithm for the detection and classification of patients with CKD. Adapted from Kidney Health Australia.13
* The decision to refer a patient with CKD to a nephrologist should be made on a case-by-case basis. For some patients (e.g. a stable eGFR < 30 mL/min/1.73 m2), nephrology advice may be all that is required along with continued management in primary care.
Evaluating eGFR and urine ACR results
 Reduced eGFR. If a patient’s eGFR is < 60 mL/min/1.73 m2, serum creatinine should be repeated within two weeks, and again in three months (or more frequently as required); Figure 1.1, 13, 18 Small variations in eGFR are possible and measurements in isolation are not always indicative of kidney disease.1, 13 If a patient has at least two eGFR results < 60 mL/min/1.73 m2 over a three month period or longer (irrespective of their urine ACR), this is supportive of a diagnosis of CKD.13 N.B. Serum creatinine within normal parameters does not exclude the possibility of CKD; kidney function decreases of ≥ 50% can occur before serum creatinine exceeds the upper limit of normal.13
Reduced eGFR. If a patient’s eGFR is < 60 mL/min/1.73 m2, serum creatinine should be repeated within two weeks, and again in three months (or more frequently as required); Figure 1.1, 13, 18 Small variations in eGFR are possible and measurements in isolation are not always indicative of kidney disease.1, 13 If a patient has at least two eGFR results < 60 mL/min/1.73 m2 over a three month period or longer (irrespective of their urine ACR), this is supportive of a diagnosis of CKD.13 N.B. Serum creatinine within normal parameters does not exclude the possibility of CKD; kidney function decreases of ≥ 50% can occur before serum creatinine exceeds the upper limit of normal.13
An eGFR reduction of ≥ 20% between measurements may indicate acute kidney injury; discuss the patient with, or refer to, a nephrologist as required (see: “Preventing acute kidney injury in patients with CKD”).1, 13
 Elevated urine ACR. If a patient’s urine ACR is ≥ 3 mg/mmol, repeat the test in three months (Figure 1).13 If the urine ACR is normal (i.e. < 3 mg/mmol) at the three-month mark, a third test is recommended. If a patient has at least two urine ACR results ≥ 3 mg/mmol over a three month period or longer (irrespective of their eGFR), this is supportive of a diagnosis of CKD.13
Elevated urine ACR. If a patient’s urine ACR is ≥ 3 mg/mmol, repeat the test in three months (Figure 1).13 If the urine ACR is normal (i.e. < 3 mg/mmol) at the three-month mark, a third test is recommended. If a patient has at least two urine ACR results ≥ 3 mg/mmol over a three month period or longer (irrespective of their eGFR), this is supportive of a diagnosis of CKD.13
Considerations when interpreting eGFR/urine ACR results
Numerous factors can influence eGFR and urine ACR results other than CKD (Table 2), and these should always be considered, particularly for patients with borderline or isolated abnormalities.
Table 2. Examples of factors that can influence eGFR and urine ACR results.1, 13
| eGFR |
Overestimation (i.e. factors that decrease serum creatinine resulting in an artificially high eGFR; true GFR likely to be lower)
- Low skeletal muscle mass, e.g. anorexia nervosa, paraplegics, amputees
- Vegan/vegetarian diet (red meat is a major source of creatinine)
- Liver disease
Underestimation (i.e. factors that increase serum creatinine resulting in an artificially low eGFR; true GFR likely to be higher)
- High consumption of red meat
- Creatine supplementation
- High muscle mass
- Medicines that limit creatinine excretion, e.g. trimethoprim
- Pregnancy
- Age < 18 years
|
| Urine ACR |
Overestimation (i.e. factors that increase urine albumin excretion; true urine ACR likely to be lower)
- Urinary tract infection
- Fever
- Menstruation
- Intense exercise
- Medicines, e.g. NSAIDs
Underestimation (i.e. factors that increase urinary creatinine excretion; true ACR likely to be higher)
|
Identify the underlying cause of CKD: other tests to request
Full classification of CKD requires consideration of the underlying cause, in addition to eGFR and persistent albuminuria category. The cause may be apparent from the patient’s history or further investigation will be required.1
Additional investigations may include:1, 8
- Dipstick urinalysis to detect haematuria or pyuria; if positive, send the urine sample for microscopy, e.g. to detect dysmorphic red cells, red and white cell casts or crystals
- Laboratory investigations, e.g. full blood count, CRP, HbA1c, lipids, urate, electrolytes, albumin
- Kidney ultrasound – see community referred radiology guidelines for criteria
- Other relevant tests according to patient-specific risk factors and clinical suspicion
Best Practice Tip. Ensure CKD is appropriately coded in the patient’s clinical record (i.e. cause, eGFR and persistent albuminuria [CGA] category). Coded CKD is associated with positive outcomes, including improved blood pressure control and prescribing practices (e.g. fewer prescriptions for NSAIDs, fewer dosing errors).7
Assess the risk of kidney failure and CVD
The use of eGFR and persistent albuminuria categorisation (Table 1) can provide broad predictive information around patient prognosis and the need for referral. However, in addition to this, the use of CKD risk prediction equations are recommended for patients with CKD G3 – 5 to more accurately assess their absolute risk of kidney failure.1
The most commonly recommended kidney failure risk calculator is The Kidney Failure Risk Equation (KFRE); a five-year risk of kidney failure of > 3 – 5% usually indicates a need for secondary care advice or referral.1, 20 Other prognostic tools for absolute risk prediction include: Risk for 40% GFR decline, Predicting Risk for CVD Events (PREVENT) and Advanced CKD Risk Tool.20 These tools have been validated in international cohorts, primarily in North America and Europe.20 Despite their strong predictive value, the applicability to the New Zealand population (including Māori and Pacific peoples who have a high burden of CKD) is not fully understood. N.B. New Zealand CVD risk equations are available that incorporate kidney function and give an estimate of end-stage kidney disease risk, but only apply to patients with co-morbid diabetes.
Assessing CVD risk in patients with CKD
CVD risk assessment tools can be used in patients with an eGFR ≥ 30 mL/min/1.73 m2; patients with an eGFR < 30 mL/min/1.73 m2 are considered to have a CVD risk equivalent to those with established CVD (i.e. five-year CVD risk > 15%) and therefore, do not require separate CVD risk assessment.21
KDIGO guidelines recommend CVD risk assessment calculators that incorporate eGFR and albuminuria as this helps to more accurately gauge overall CVD risk, or one that has been validated within a CKD population.1 In New Zealand, CVD risk calculators tailored for use in people with diabetes often include urine ACR and eGFR, however, others intended for more general use (i.e. irrespective of diabetes status) typically do not.
For further information on CVD risk assessment in primary care, see: https://bpac.org.nz/2018/cvd.aspx
Patients requiring nephrologist referral
The decision to refer a patient with CKD to a nephrologist should be made on a case-by-case basis. For some patients (e.g. stable eGFR < 30 mL/min/1.73 m2), formal referral involving consultation and ongoing monitoring with a nephrology service may not be necessary; nephrology advice may be all that is required along with continued management in primary care. A lower threshold for referral may be appropriate for patients who are younger or of Māori or Pacific ethnicity. Include the patient’s CKD CGA classification on the referral.
Check local HealthPathways for region-specific referral protocols. In general, discussion with, or referral to, a nephrologist is recommended for patients with:1, 3, 13
- An eGFR < 30 mL/min/1.73 m2 or < 45 mL/min/1.73 m2 if they have diabetes and persistent urine ACR > 30 mg/mmol
- A sustained decrease in eGFR of 10 – 15 mL/min/1.73 m2 or ≥ 25% and a change in eGFR category within 12 months, or change in eGFR of ≥ 20% between measurements
- Persistent macroalbuminuria (i.e. urine ACR > 30 mg/mmol) in combination with haematuria, or urine ACR > 70 mg/mmol
- An uncertain or unclear cause of CKD
- Hereditary kidney disease
- Recurrent extensive nephrolithiasis
- Suspected intrinsic kidney damage (e.g. glomerulonephritis) or renal artery stenosis
- Five-year risk of kidney replacement > 3 – 5%
 Urgently refer patients with a rapidly declining eGFR (> 5 mL/min/1.73 m2 over three months) or symptoms and signs of acute nephritis (e.g. oliguria, haematuria, acute hypertension).13
Urgently refer patients with a rapidly declining eGFR (> 5 mL/min/1.73 m2 over three months) or symptoms and signs of acute nephritis (e.g. oliguria, haematuria, acute hypertension).13
The majority of patients with stable CKD can be fully managed in primary care, particularly if they have stable CKD G3 or are aged over 75 years with early stable CKD G4.3 Patients will likely have other co-morbidities, e.g. diabetes, hypertension, that share common management strategies and priorities.
The main goals of CKD management are to slow the progressive loss of kidney function and to reduce the associated CVD risk.13, 19 This is achieved through a combination of lifestyle changes and pharmacological management targeting albuminuria, blood pressure and hyperglycaemia (if the patient has diabetes), or an alternative underlying cause. Albuminuria is a significant modifiable risk factor for CKD progression and CVD; small changes in albuminuria have a greater effect on CKD progression and CVD risk than small reductions in eGFR.7, 13
Software-based decision support, audit and patient recall systems are an important part of best practice in the management of CKD.3 If you do not have CKD decision support software installed in your practice management system, contact BPAC Clinical Solutions for information about their CKD module.
Community-based care strategies, involving nurse-led teams and healthcare assistants have also been shown to improve the management of patients with CKD, including in a primary care setting.3, 22 Therefore, consider how all members of the primary care team can be involved in the management of patients with CKD.
Consider reversible causes of kidney function decline
In some cases, a reversible cause of CKD may be present in patients who have been recently diagnosed or be the driver of acute deterioration in those with established CKD. If corrected, this may lead to recovery of kidney function. Examples include dehydration, hypotension, nephrotoxic medicine use, e.g. NSAIDs, and urinary tract obstruction.13, 18
CKD is a prominent risk factor for gout
Declining kidney function limits urate clearance, resulting in increased serum urate levels; once this passes the saturation point (0.36 mmol/L), monosodium urate crystal deposition can occur in joints, resulting in gout symptoms for some people.1, 23 Up to 70% of people with gout have an eGFR < 60 mL/min/1.73 m2, and gout further increases CVD risk in people with CKD.23 As with CKD, the prevalence of gout increases with age and rates are significantly higher for Māori and Pacific peoples.24
Urate-lowering treatment is indicated in patients with CKD who have symptomatic hyperuricaemia; kidney dysfunction alone is not an indication for urate-lowering treatment in the absence of a gout flare.1, 13 Monitoring kidney function in patients with CKD and gout is particularly important as many of the medicines used to treat gout, e.g. allopurinol, colchicine, are potentially nephrotoxic, and dosing decisions are based on the patient’s eGFR.13, 25
For further information on gout management, see: https://bpac.org.nz/2025/gout.aspx
Lifestyle modifications are an important component of management for all patients with CKD (or at risk) to help to slow progression to advanced CKD and reduce cardio-renal-metabolic risk.13 Ensure that recommendations are appropriately tailored to each patient, including cultural considerations, as this can sometimes be a barrier to engagement.26
Key examples of lifestyle changes include:1, 13
 Weight management. Reducing BMI to a target of < 25 kg/m2 (< 23 kg/m2 for Asian populations) is ideal; however, any reduction in weight is beneficial. Central obesity is a risk factor for albuminuria and CKD progression; a waist circumference for males of < 94 cm (< 90 cm for Asian males) and for females < 80 cm (including Asian females) should be targeted.
Weight management. Reducing BMI to a target of < 25 kg/m2 (< 23 kg/m2 for Asian populations) is ideal; however, any reduction in weight is beneficial. Central obesity is a risk factor for albuminuria and CKD progression; a waist circumference for males of < 94 cm (< 90 cm for Asian males) and for females < 80 cm (including Asian females) should be targeted.
For further information on weight loss, see: https://bpac.org.nz/2022/weight-loss.aspx
 Exercise. Engage in at least 150 minutes per week of moderate-intensity physical activity (or to a level that is tolerable). Strength/resistance training is advised at least twice per week, e.g. lifting weights, using a resistance band, stair climbing.
Exercise. Engage in at least 150 minutes per week of moderate-intensity physical activity (or to a level that is tolerable). Strength/resistance training is advised at least twice per week, e.g. lifting weights, using a resistance band, stair climbing.
 Nutrition. Recommend a balanced diet that emphasises intake of vegetables, fruits, nuts, low-fat dairy products, whole grains, lean meat and fish, e.g. the DASH diet. In addition:
Nutrition. Recommend a balanced diet that emphasises intake of vegetables, fruits, nuts, low-fat dairy products, whole grains, lean meat and fish, e.g. the DASH diet. In addition:
- Reduce sodium intake to < 2 g per day (equivalent to less than one teaspoon of salt). Avoid adding salt to meals, and select reduced-salt packaged food products, where possible.
- Avoid consumption of trans fats and minimise intake of processed meats, refined carbohydrates and sugar-sweetened beverages
- Drink water to satisfy thirst but avoid overconsumption
- Avoid high-protein diets (> 1.3 g/kg/day) and creatine supplements. The suitability of protein restriction continues to be debated in the literature and is not routinely recommended (see: “The jury remains out on low-protein diets”).
 Reducing alcohol consumption. There is no specific recommendation about alcohol consumption for people with CKD (other than standard advice), but the less people drink, the lower the risk of harm.
Reducing alcohol consumption. There is no specific recommendation about alcohol consumption for people with CKD (other than standard advice), but the less people drink, the lower the risk of harm.
For further information on alcohol, see: bpac.org.nz/2018/alcohol.aspx
 Smoking/vaping cessation (if relevant). Smoking is a risk factor for CKD progression and vaping has been associated with albuminuria; therefore, smoking and vaping cessation should be a priority. Smoking cessation may decrease albuminuria and slow CKD progression in people with CKD.27
Smoking/vaping cessation (if relevant). Smoking is a risk factor for CKD progression and vaping has been associated with albuminuria; therefore, smoking and vaping cessation should be a priority. Smoking cessation may decrease albuminuria and slow CKD progression in people with CKD.27
For further information on smoking cessation, see: bpac.org.nz/2024/smoking.aspx
The jury remains out on low-protein diets
One of the most extensively studied dietary interventions for CKD is protein restriction, however, investigations have yielded mixed results.28 Protein restriction is proposed to reduce progression of CKD in part by reducing glomerular hyperfiltration.28, 29 In most cases, a normal protein intake (i.e. 0.8 g/kg/day) is encouraged for people with CKD, and a low-protein diet (i.e. ≤ 0.6 g/kg/day) is advised against as insufficient dietary protein can lead to malnutrition, particularly in older people.1, 18, 28
The Kidney Disease Outcomes Quality Initiative (KDOQI) clinical guideline for nutrition in CKD (2020) recommends, under close supervision, a low-protein diet (0.55 – 0.6 g/kg/day) or very-low protein diet (0.3 – 0.4 g/kg/day with additional essential amino acid or ketoacid analogue supplementation) for people with CKD G3 – 5 who are metabolically stable (without diabetes and not undergoing dialysis) to reduce the risk of end-stage kidney disease/mortality and improve quality of life.30 For people with diabetes and CKD G3 – 5, a more lenient protein intake of 0.6 – 0.8 g/kg/day may be reasonable to maintain nutrient status and optimise glycaemic control.30
A dietary protein intake of 0.6 g/kg/day equates to 48 g of protein for an 80 kg person per day, e.g. approximately 170 g of fillet steak, 150 g chicken breast or 190 g of canned tuna. Other sources of protein, such as soy, grains, nuts and pulses also contribute to total intake and should be factored in when reviewing protein options. Vegetable-derived proteins may induce lower levels of glomerular hyperfiltration than animal-derived protein, and may be more suitable in certain situations, e.g. patients with hyperphosphataemia.29
A low- or very-low protein diet is not standard practice in New Zealand for patients with CKD and should only be considered under the guidance of a nephrologist or dietitian.
For information on the nutritional content of foods, see: https://www.foodcomposition.co.nz/

All patients newly diagnosed with CKD should have their current medicines reviewed for potential nephrotoxicity, e.g. NSAIDs, lithium, aminoglycoside antibiotics; consider whether dose adjustments, switching or discontinuation is required.1, 13 Also consider use of over-the-counter products, as well as complementary or alternative medicines. Decisions around nephrotoxic medicines can sometimes be challenging in the setting of CKD; while they may contribute to further deteriorating kidney function, some are essential for pre-existing conditions. If there is uncertainty, seek further advice, e.g. from a clinical pharmacist facilitator or nephrologist.
Traditional remedies: There are several traditional Rongoā Māori treatments for kidney and urinary complaints, e.g. Kawakawa (pepper tree), Karamū (Coprosma robusta), Manuka and Kānuka (tea-tree). Patients should generally be supported in the use of traditional healing remedies when there is no evidence for harm, but advise stopping use if there is suspicion of nephrotoxicity or possible interactions with other conventional medicines.
The “four pillars” of CKD management
A combination of medicines, termed the “four pillars” approach, is increasingly being recognised as the new standard of care for managing patients with CKD, particularly those with co-morbid diabetes, similar to what is now considered standard practice for heart failure.
The “four pillars” of CKD treatment are:20, 31
- An angiotensin-converting enzyme (ACE) inhibitor/angiotensin-II receptor blocker (ARB); and
- A sodium-glucose co-transporter 2 (SGLT-2) inhibitor; and/or
- A glucagon-like peptide-1 (GLP-1) receptor agonist; and/or
- A non-steroidal mineralocorticoid receptor antagonist (MRA)
This approach works by targeting different aspects of the cardio-renal system to reduce albuminuria, blood pressure and optimise glycaemic control (as needed), and therefore, reduce progression of CKD and cardio-renal-metabolic risk.14 Some of these medicines work in tandem to improve safety and tolerability of the overall regimen, e.g. ACE inhibitors/ARBs raise serum potassium levels, but SGLT-2 inhibitors can reduce the risk of hyperkalaemia.14, 20 Other medicines can also be added to the patient’s treatment regimen as needed, e.g. lipid-lowering medicines.
The benefits of combination treatment have primarily been demonstrated in people with CKD and diabetes, however, evidence in those without diabetes is increasing, particularly for SGLT-2 inhibitors.20, 31 The absolute benefits of combination treatment with all four medicines in patients with CKD are greatest in those at high risk of progression to advanced CKD, e.g. those with significantly reduced eGFR or albuminuria;20 this differs to heart failure, where the introduction of all “four pillars” is recommended promptly for most patients irrespective of disease severity. Further research is required to determine the optimal timing and intensity of the “four pillars” treatment across all patient groups with CKD, e.g. those at lower risk of progression.20 However, international evidence suggests that the “four pillars” are underutilised among people with CKD who need them the most.20
Applying the “four pillars” approach in primary care in New Zealand
In New Zealand, medicines availability and Special Authority funding restrictions influence the ability to adopt the “four pillars” approach. SGLT-2 inhibitors and GLP-1 receptor agonists are not funded for patients with CKD unless they have other co-morbidities (e.g. diabetes or heart failure). However, the option of self-funding treatment should still be discussed, so patients can consider it depending on their individual circumstances. There are no non-steroidal MRAs routinely available in New Zealand (except in a clinical trial setting).
Prescribing decisions can be made using a risk-based approach, prioritising the addition of key medicines to the patient’s regimen where possible.
All patients with CKD should be taking an ACE inhibitor or ARB
An ACE inhibitor or ARB is recommended first-line for patients with CKD, particularly when albuminuria is present, for their antiproteinuric effect and blood pressure control which can slow the rate of CKD progression and reduce CVD risk.1, 8, 13 ACE inhibitors and ARBs are considered to be similarly effective;20 in practice, an ARB is often preferred due to the lower risk of adverse effects. Concurrent use is not recommended in clinical guidelines.1
Once initiated, the medicine should be up-titrated to the maximum (approved) tolerated dose.1, 13 Aim for an overall blood pressure target of < 120 – 130/80 mmHg, individualised to the patient, e.g. consider less intensive targets for patients with frailty or high risk of falls, and more assertive targets for patients at higher risk of CKD progression or CVD.1, 7
Monitor for changes in serum creatinine and potassium
Monitor patients for acute changes in serum creatinine and potassium – ideally two to four weeks after initiation of an ACE inhibitor/ARB or an increase in dose.1, 13
An increase in serum creatinine of up to 30% or a reduction in eGFR of up to 25% within four weeks following treatment initiation or a dose increase is considered clinically acceptable; consider reducing the dose or discontinuing the medicine if changes above these values occur.1, 13
An increase in serum potassium of approximately 0.5 mmol/L is usually expected with ACE inhibitor/ARB use and in the context of CKD, a serum potassium level of up to 6.0 mmol/L is considered acceptable.13 If a patient develops hyperkalaemia, ideally manage with dietary and pharmacological measures rather than reducing the dose or stopping the ACE inhibitor/ARB.1 For example, reduce dietary potassium intake, stop or switch any medicines and supplements that raise serum potassium, e.g. beta blocker (unless it will compromise management of any co-morbidities), prescribe a diuretic, e.g. furosemide, to increase potassium excretion.1, 14 Adding empagliflozin might enable patients to continue taking an ACE inhibitor/ARB as the risk of hyperkalaemia is lower with concomitant ACE inhibitor/ARB and SGLT-2 inhibitor use (see: “Initiate empagliflozin, where possible”).14, 20 Patients with persistent hyperkalaemia usually require discussion with, or referral to, a nephrologist.1
Escalate antihypertensive treatment as needed: add a calcium channel blocker, diuretic or beta blocker
Multiple antihypertensives will generally be required to achieve blood pressure control in patients with CKD. Adding a dihydropyridine calcium channel blocker (e.g. amlodipine) or diuretic (thiazide or loop) is a suitable next step.1, 13 A beta blocker may be considered for combination treatment, particularly if patients have other co-morbidities, e.g. heart failure.13 For patients with resistant hypertension and an eGFR of ≥ 45 mL/min/1.73 m2, a steroidal MRA, e.g. spironolactone, may be required.1 Nephrology referral is usually indicated if the patient’s blood pressure is not controlled with multiple antihypertensives.1, 13
Initiate empagliflozin, where possible
There is increasing evidence and emphasis on the use of SGLT-2 inhibitors in CKD management, in addition to their role in type 2 diabetes.20, 31 In people with CKD (with or without diabetes), SGLT-2 inhibitors have been reported to decrease kidney disease progression, reduce acute kidney injury, decrease CVD risk, hospitalisations due to heart failure and all-cause mortality.6, 14, 32
A SGLT-2 inhibitor is recommended to be added to an ACE inhibitor/ARB for all patients with CKD and an eGFR ≥ 20 mL/min/1.73 m2 who have:1
- Type 2 diabetes; or
- Moderately increased albuminuria (urine ACR ≥ 20 mg/mmol)*; or
- Heart failure
* If urine ACR is < 20 mg/mmol in a patient with an eGFR 20 – 45 mL/min/1.73 m2, a SGLT-2 inhibitor is suggested in KDIGO guidelines
Empagliflozin (with and without metformin) is the only SGLT-2 inhibitor routinely prescribed in New Zealand (dapagliflozin is also available; not funded). Under current Special Authority funding criteria, empagliflozin is only funded for patients with CKD if they also have type 2 diabetes or heart failure with reduced ejection fraction (see Special Authority criteria here). This may present a barrier to equitable access as patients who do not meet these criteria will need to self-fund treatment. This option should be discussed with patients, so they have the opportunity to consider it depending on their individual circumstances.
Empagliflozin: key prescribing information
 Dosing. The lowest available strength of empagliflozin (i.e. 10 mg, daily) is recommended for patients with CKD, as a dose-response relationship for cardio-renal outcomes has not been observed.33 10 mg, daily, is also the maximum approved dose of empagliflozin for patients with an eGFR < 30 mL/min/1.73 m2.25 Empagliflozin is not recommended to be initiated in patients with an eGFR < 20 mL/min/1.73 m2 due to limited safety and efficacy data, however if the eGFR drops below this value during treatment, the medicine can be continued until kidney transplant or dialysis (unless it is not tolerated).1, 25
Dosing. The lowest available strength of empagliflozin (i.e. 10 mg, daily) is recommended for patients with CKD, as a dose-response relationship for cardio-renal outcomes has not been observed.33 10 mg, daily, is also the maximum approved dose of empagliflozin for patients with an eGFR < 30 mL/min/1.73 m2.25 Empagliflozin is not recommended to be initiated in patients with an eGFR < 20 mL/min/1.73 m2 due to limited safety and efficacy data, however if the eGFR drops below this value during treatment, the medicine can be continued until kidney transplant or dialysis (unless it is not tolerated).1, 25
In patients with CKD with co-morbid type 2 diabetes, the dose of empagliflozin can be increased to 25 mg, daily, if HbA1c remains above target and their eGFR is ≥ 30 mL/min/1.73 m2. Empagliflozin may be ineffective for glycaemic control in patients with an eGFR < 30 mL/min/1.73 m2 and additional glucose-lowering medicines needed (see: “Prescribe a GLP-1 receptor agonist to patients with co-morbid diabetes”).25, 33
A transient reduction in eGFR is expected when initiating a SGLT-2 inhibitor, but this is not a reason to discontinue treatment.1, 13
 Other considerations. SGLT-2 inhibitors are associated with:
Other considerations. SGLT-2 inhibitors are associated with:
- An increased risk of ketoacidosis; risk is higher in people with diabetes and during an acute illness25, 34
- An increased risk of genital mycotic infections; these can be treated with an antifungal medicine34
- There is mixed evidence as to whether SGLT-2 inhibitors increase the risk of other genitourinary infections, e.g. urinary tract infection; most data do not support an association33, 34
- Ensure patients are given information on hygiene measures and the rare risk of necrotising fasciitis of the perineum (Fournier’s gangrene), and be advised to seek immediate medical attention if they have pain, tenderness, erythema or swelling of the genital or perineal area25, 34
- Osmotic diuresis; it may be appropriate to reduce the dose of medicines with a diuretic effect to lower the risk of volume depletion13, 33
- An increase in potassium excretion; this may allow for up-titration or continued use of an ACE inhibitor/ARB33
Best Practice Tip: For patients who are self-funding empagliflozin, consider ways to reduce cost for them, e.g. use of a disability allowance if applicable, checking costs of tablets of different strengths and between pharmacies.
Coming soon: An article focused on SGLT-2 inhibitors, including pharmacology, indications and evidence of benefit, contraindications and cautions, how to prescribe, and adverse effects is in development and due to be published soon.
Prescribe a GLP-1 receptor agonist to patients with co-morbid diabetes
One in three people with diabetes will develop CKD.13 The initial approach to glycaemic control in most people with CKD and diabetes is lifestyle changes plus metformin and a SGLT-2 inhibitor (see: “Diabetes management in CKD: HbA1c targets and metformin dosing”).35 For patients whose HbA1c is not adequately controlled with metformin and/or a SGLT-2 inhibitor (or who are unable to tolerate these medicines), a GLP-1 receptor agonist is recommended (if eGFR is ≥ 15 mL/min/1.73 m2).1, 35 In addition to their glucose-lowering effects, GLP-1 receptor agonists have been reported to improve CKD outcomes, e.g. reduce CKD progression, and CVD risk, e.g. myocardial infarction, as well as induce weight loss.6, 7, 31
More studies are needed to determine the role of GLP-1 receptor agonists in CKD management for people without diabetes, but emerging evidence suggests a benefit with semaglutide in those who are overweight/obese.20, 31 CKD is an approved indication for semaglutide in some countries, e.g. Australia, United States of America, but currently not in New Zealand.
Prescribing considerations
In New Zealand, GLP-1 receptor agonists are indicated for:
- Type 2 diabetes (dulaglutide, liraglutide, semaglutide, tirzepatide)
- Cardiovascular event risk reduction in people with type 2 diabetes and established CVD or multiple risk factors (dulaglutide, liraglutide)
- Cardiovascular risk reduction in people with established CVD and a BMI > 27 kg/m2 without diabetes (semaglutide)
- Adjunctive treatment for weight management in people with a BMI ≥ 30 kg/m2, or in people with a BMI ≥ 27 kg/m2 who have at least one weight-related co-morbidity (liraglutide, semaglutide, tirzepatide)
Dulaglutide and liraglutide are funded with Special Authority approval only for patients with diabetes, and dual SGLT-2 inhibitor/GLP-1 receptor agonist treatment is not funded (unless the patient has co-morbid heart failure). Other GLP-1 receptor agonists are not funded.
Best Practice Tip: For patients with CKD and co-morbid type 2 diabetes and heart failure, apply for funded empagliflozin under the Special Authority for heart failure and funded dulaglutide/liraglutide under the Special Authority for diabetes if the patient’s HbA1c remains above target.
Nausea and diarrhoea are common with GLP-1 receptor agonists.7 To reduce the likelihood of gastrointestinal adverse effects, initiate treatment at a low dose and up-titrate slowly.7
For further information on GLP-1 receptor agonists, see: bpac.org.nz/2021/diabetes.aspx and https://t2dm.nzssd.org.nz/Section-82-GLP-1-receptor-agonists--GLP1RA-
Diabetes management in CKD: HbA1c targets and metformin dosing
A HbA1c target of ≤ 53 mmol/mol (range 48 – 64 mmol/mol) is generally appropriate for patients with CKD and type 2 diabetes, but more lenient targets can be considered depending on individual circumstances, e.g. multiple co-morbidities, limited life expectancy.13, 16, 35 A less intensive target may also be appropriate for patients with more advanced CKD, given that hypoglycaemia becomes more common as eGFR decreases.13, 35
Metformin is a first-line medicine for glycaemic control in patients with CKD; the maximum dose depends on the patient’s kidney function (Table 3).35 KDIGO guidelines recommend both metformin and a SGLT-2 inhibitor first-line for patients with type 2 diabetes and CKD,35 however, in New Zealand a SGLT-2 inhibitor is usually second line for glycaemic control due to Special Authority funding restrictions. Alternative glucose-lowering medicines include vildagliptin, pioglitazone (except in heart failure), a sulfonylurea or insulin.13, 36
Table 3. Maximum daily dose of metformin based on eGFR.25, 36
| eGFR (mL/min/1.73 m2)* |
Maximum metformin dose per day |
| 60 – 120 |
2 g |
| 30 – 60 |
1 g
N.B. KDIGO guidelines for diabetes management in CKD (2022) recommend that a metformin dose of up to 2 g, daily, is safe when eGFR is > 45 mL/min/1.73 m2.35 The New Zealand Society for the Study of Diabetes advises that best practice is now to only reduce the dose of metformin when the eGFR is < 45 mL/min/1.73 m2 (this recommendation is off-label but widely adopted).36 |
| 15 – 30 |
0.5 g |
| < 15 |
Contraindicated |
* While in many cases eGFR will be sufficient to estimate kidney function in patients taking metformin, the Manufacturer advises using creatinine clearance, calculated from the Cockcroft and Gault equation, to estimate kidney function25
For further information on type 2 diabetes management, see: bpac.org.nz/2021/diabetes-management.aspx
Non-steroidal mineralocorticoid receptor antagonists: not routinely available in New Zealand
Non-steroidal MRAs are not approved nor readily available in New Zealand and therefore, they do not form part of routine management for patients with CKD. In international guidelines, they are an integral part of the “four pillars” approach for people with CKD (with an eGFR > 25 mL/min/1.73 m2) and diabetes who have persistent albuminuria (> 3 mg/mmol) despite taking the maximum tolerated dose of an ACE inhibitor/ARB.1, 13 Non-steroidal MRAs have been reported to reduce CKD progression and CVD risk.14, 20 Studies are ongoing to evaluate non-steroidal MRAs in people with non-diabetic kidney disease.20 A non-steroidal MRA is currently being studied in New Zealand as part of the CAPTIVATE trial.
Steroidal MRAs (e.g. spironolactone, eplerenone) are available and funded in New Zealand, but are not a suitable substitute for patients in whom a non-steroidal MRA is recommended.14 A steroidal MRA could be considered for patients with CKD and co-morbid heart failure, hyperaldosteronism or resistant hypertension, but caution is required due to the risk of hyperkalaemia and a reversible decline in glomerular filtration.1, 13
Additional medicines to consider
Lipid management. Dyslipidaemia is common in people with CKD, particularly high triglyceride levels and low HDL-C, and is generally more severe in those with albuminuria.13, 37 CARI guidelines recommend initiating a statin, with or without ezetimibe, to reduce cardiovascular events and mortality in people with CKD (eGFR ≥ 15 mL/min/1.73 m2) and a CVD risk ≥ 10% (or ≥ 5% if Māori ethnicity).37 Given the high risk of CVD associated with CKD, the benefits of lipid-lowering treatment should be discussed with those who have a CVD risk of 5 – 10%.37 Some patients with CKD regardless of their calculated CVD risk will also benefit from a statin (with or without ezetimibe), e.g. patients with persistent albuminuria.37 In practice, atorvastatin is usually first-line, unless the patient meets Special Authority criteria for rosuvastatin.
Aspirin. In general, long-term use of low-dose aspirin should be considered for secondary prevention in patients with CKD and established CVD.1, 35 The evidence for aspirin for primary prevention in patients with CKD at high risk of atherosclerotic events is uncertain; therefore it is not routinely recommended for this purpose.1
Preventing acute kidney injury in patients with CKD
People with CKD have an increased risk of developing acute kidney injury, which is characterised by a rapid reduction in GFR.1, 13 Medicines are a common cause of acute kidney injury and people with an acute dehydrating illness (e.g. gastrointestinal illness, infection causing hypovolaemia) are at significant risk.1,13
Some medicines should be used with caution in patients with CKD. For example, the “triple whammy” of NSAIDs, ACE inhibitors (or ARBs) and diuretics can result in acute kidney injury.13 Adequate fluid intake and electrolyte maintenance are important to maintain blood/plasma volume in people with CKD who are acutely unwell.13
The mnemonic SADMANS can be used as a reminder of which medicines should be withheld during an acute illness:1, 13
- Sulfonylureas
- ACE inhibitors
- Diuretics
- Metformin
- ARBs
- NSAIDs
- SGLT-2 inhibitors
The medicine(s) should be recommenced once the patient has recovered from the acute illness.1, 13
People with CKD are also at increased risk of developing acute kidney injury if they undergo procedures involving radiocontrast material; it may be necessary to temporarily withdraw potentially nephrotoxic medicines prior to the procedure.1 The use of metformin is contraindicated in people undergoing procedures involving iodine-containing X-ray contrast media, e.g. angiography, due to an increased risk of lactic acidosis (particularly in those with renal impairment).25
A patient resource with sick day advice is available from: https://healthed.govt.nz/products/kidney-health-at-home-sick-day-advice-he2647
Patients with CKD require ongoing review to assess for progression to advanced CKD and the development of complications (see below), and to optimise their treatment regimen if co-morbidities are not adequately controlled, e.g. diabetes, hypertension.3, 13 It is also an opportunity to reinforce positive lifestyle changes, and assess general wellbeing; depression is common in people with CKD.13
The patient’s eGFR and urine ACR should be assessed at least annually.1, 13 The frequency of review is guided by CKD severity and the presence of co-morbidities,1, 13 e.g. patients with progressive CKD G3 – 4 have a much greater risk of developing kidney failure and usually require intensive management with review and risk factor management every one to two weeks until their condition is stable.3 Table 4 provides a suggested monitoring schedule for patients with CKD according to severity.
Table 4. Suggested monitoring and investigation schedule for patients with CKD.13
| CKD parameters |
Frequency of review |
Laboratory investigations |
Clinical assessment |
- eGFR ≥ 60 mL/min/1.73 m2 with microalbuminuria (A2) or
- eGFR 45 – 59 mL/min/1.73 m2 with normal albumin (A1)
|
|
Recommended:
- Creatinine (eGFR)
- Urine ACR
- Urea
- Electrolytes
- Full blood count
N.B. Urea is not often tested in a primary care setting, but if disproportionately elevated compared to creatinine, it may suggest causes such as corticosteroid use, increased protein breakdown or gastrointestinal bleeding, rather than true kidney function decline.
Consider:
- HbA1c
- Lipid panel
- Iron studies
- Dipstick urinalysis for haematuria
|
- Blood pressure
- Weight and waist circumference
- Smoking/vaping status
- Medicine use; avoid nephrotoxic options and adjust doses depending on kidney function
- Check for oedema (if macroalbuminuria irrespective of eGFR or eGFR < 30 mL/min/1.73 m2 irrespective of albuminuria)
|
- eGFR 30 – 59 mL/min/1.73 m2 with microalbuminuria (A2) or
- eGFR 30 – 44 mL/min/1.73 m2 with normal albumin (A1)
|
- Every three to six months
|
- In addition to above, consider:
- Calcium and phosphate
- Parathyroid hormone
- Albumin
N.B. Albumin can be requested alone or as part of a LFT panel. Low serum albumin can occur with nephrotic range proteinuria (ACR > 300 mg/mmol) and nephrotic syndrome (oedema, ACR < 300 mg/mmol). |
|
- Macroalbuminuria irrespective of eGFR or
- eGFR < 30 mL/min/1.73 m2 irrespective of albuminuria
|
- Every one to three months
|
As CKD progresses, patients can develop a range of complications, such as metabolic acidosis and bone disease, anaemia, malnutrition, infection risk and acute kidney injury, due to changes in kidney function and metabolism of certain hormones and minerals.1, 3, 13 The complications of advanced CKD will usually be managed by a kidney team; discuss with, or refer patients to, a nephrologist.
Check patients are up to date with recommended vaccinations
People with CKD are at higher risk with some infections, e.g. herpes zoster, Streptococcus pneumoniae.6, 38 Response to vaccination decreases as the severity of CKD increases.38
It is recommended that people with CKD receive standard vaccinations on the National Immunisation Schedule, plus they may be eligible for additional vaccinations, depending on their immunosuppression status and stage of CKD, including:13, 38
- Influenza
- COVID-19
- Pneumococcal and meningococcal
- Herpes zoster (Shingrix)
- Hepatitis A and B
- Haemophilus influenzae type b
Specific information on vaccination recommendations for people with CKD is available in the Immunisation Handbook: https://www.tewhatuora.govt.nz/for-health-professionals/clinical-guidance/immunisation-handbook/4-immunisation-of-special-groups#4-4-chronic-kidney-disease
An IMAC factsheet on immunisation recommendations for people with CKD pre-dialysis, who are undergoing dialysis or pre-/post-kidney transplant is also available: https://immune.org.nz/factsheets/immunisation-for-adults-pre-dialysis-on-dialysis-or-pre-post-kidney-transplantation
Patient and family/whānau resources
- Kidney Health New Zealand is an organisation that provides education, advocacy and support to people with CKD and their family/whānau. Resources are available on a range of topics, including blood pressure, diabetes, nutrition, water and fluid advice, sick day advice. Some resources are also available in Fijian, Niuean, Samoa, Te Ao Māori, Tokelau, Tongan and Tuvalu languages. Hardcopies of booklets can be ordered by practices free of charge.

- The Kidney Society provides information and support to people with CKD in Northland, Auckland, Waikato, Bay of Plenty, Lakes, Gisborne/Tairawhiti and Hawkes Bay regions
- The Christchurch Kidney Society supports people with CKD living in the South Island
- Healthify has patient information about CKD and kidney failure. Patient information on how to protect the kidneys and kidney disease apps are also available.





