
B-QuiCK: Chronic kidney disease (CKD)
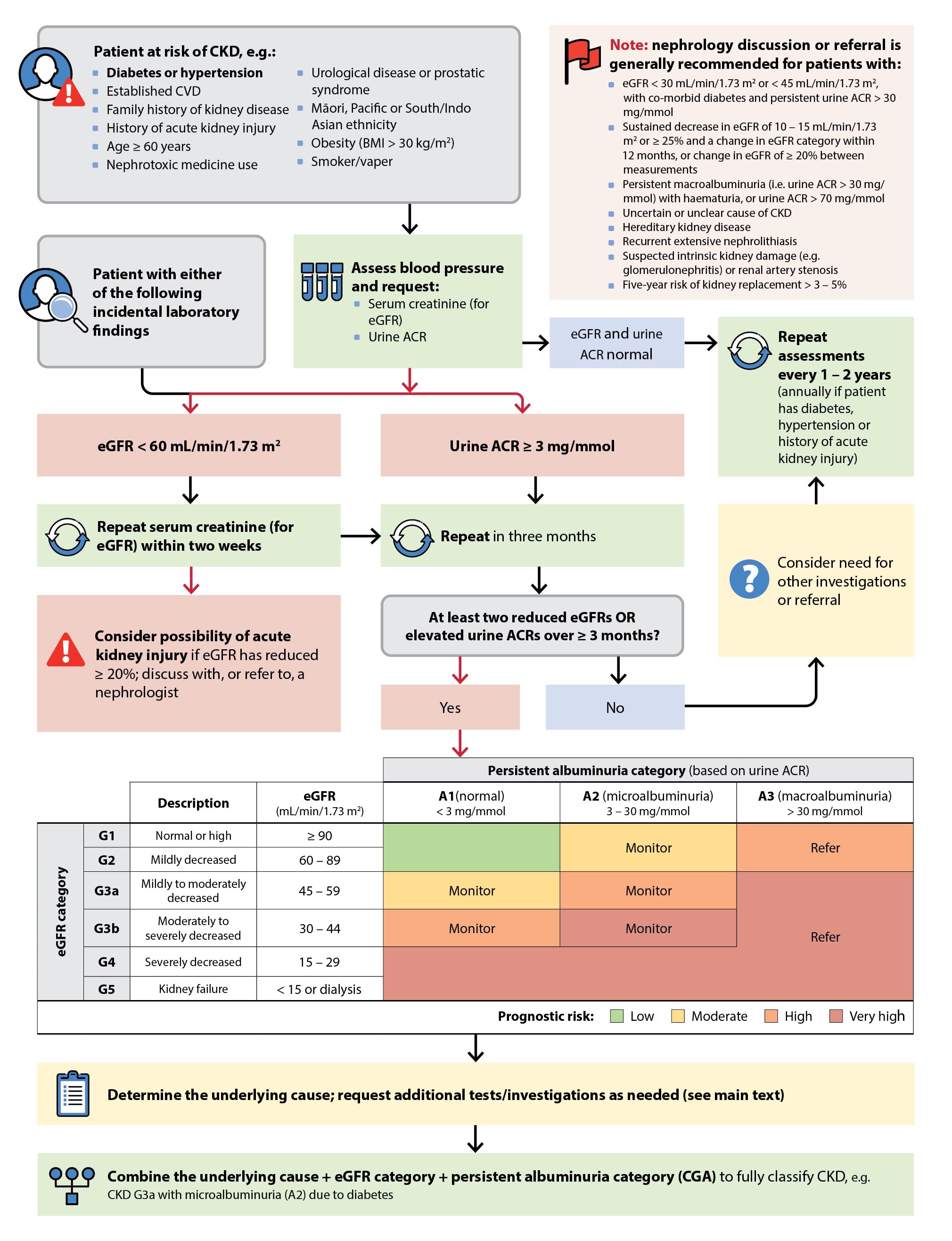
Overview of the diagnosis and classification of patients with CKD in primary care
Management of patients with CKD in primary care
Lifestyle management
| Weight loss |
- Target BMI < 25 kg/m2; but any reduction in weight is beneficial
- Target waist circumference < 94 cm for males, < 80 cm for females
N.B. Aim for lower values for people of Asian ethnicity. |
| Exercise |
- Aim for at least 150 minutes/week of moderate-intensity physical activity (or to a level that is tolerable)
- Strength/resistance training on at least two days/week
|
| Nutrition |
- Recommend a balanced diet emphasising vegetables, fruits, nuts, low-fat dairy products, whole grains and fish (e.g. DASH diet); reduce sodium intake, avoid trans fats, processed meats, refined carbohydrates, sweetened beverages. Water should be the main fluid but avoid over-consumption.
- Avoid high levels of protein intake but do not advise a protein-restricted diet unless under dietitian or nephrologist supervision
|
| Alcohol |
- No specific recommendation for people with CKD (other than standard advice), but the less alcohol consumed, the lower the risk of harm
|
| Smoking |
- Encourage smoking and vaping cessation, if applicable
|
Provide “sick day” advice. Advise patients to temporarily withhold sulfonylureas, ACE inhibitors, diuretics, metformin, ARBs, NSAIDs and SGLT-2 inhibitors during an acute illness (SADMANS).
Pharmacological management
Main goals:
- Slow progressive loss of kidney function
- Reduce CVD risk
The “four pillars” approach is becoming the new standard of care, particularly for those with diabetes and at high risk of progression to advanced CKD:
- An ACE inhibitor or ARB; and
- A SGLT-2 inhibitor; and/or
- A GLP-1 receptor agonist; and/or
- A non-steroidal mineralocorticoid receptor antagonist (not routinely available in New Zealand)
Initiate an ACE inhibitor/ARB in all patients with CKD
- Aim for BP < 120 – 130/80 mmHg for most patients
- Up-titrate the ACE inhibitor/ARB to the maximum (approved) tolerated dose
- Monitor for acute reductions in eGFR and hyperkalaemia - ideally two to four weeks after initiation or dose increase
- Serum creatinine increase up to 30% or eGFR reduction up to 25% is acceptable; reduce dose or discontinue medicine if changes above these values occur
- Serum potassium up to 6.0 mmol/L is acceptable. Manage hyperkalaemia with dietary and pharmacological measures (diuretic) before withholding or reducing the dose. Discuss or refer patients with persistent hyperkalaemia to a nephrologist.
- If antihypertensive treatment escalation is required, add a calcium channel blocker or diuretic (thiazide or loop)
Initiate empagliflozin (SGLT-2 inhibitor), where possible
- Prescribe empagliflozin 10 mg, daily (Special Authority criteria apply) for patients with an eGFR ≥ 20 mL/min/1.73 m2 who have:
- Type 2 diabetes
- Moderately increased albuminuria (urine ACR ≥ 20 mg/mmol)*
- Heart failure
- Do not initiate empagliflozin if eGFR is < 20 mL/min/1.73 m2, however, it can be continued if eGFR drops below this value during treatment (if tolerated)
- Expect a transient reduction in eGFR when initiating empagliflozin; this is not a reason for discontinuation
- Possible adverse effects include ketoacidosis, genital mycotic infections, Fournier’s gangrene (rare), osmotic diuresis
* If urine ACR is < 20 mg/mmol in a patient with an eGFR 20 – 45 mL/min/1.73 m2, a SGLT-2 inhibitor is suggested in KDIGO guidelines
Best Practice Tip: For patients who are self-funding empagliflozin, consider ways to reduce cost for them, e.g. use of a disability allowance if applicable, checking costs of tablets of different strengths and between pharmacies.
Prescribe a GLP-1 receptor agonist to patients with co-morbid diabetes
- Aim for a target HbA1C of ≤ 53 mmol/mol for most patients; ensure metformin is dosed according to eGFR (click here for dosing)
- Prescribe GLP-1 receptor agonist (dulaglutide and liraglutide are funded with Special Authority approval) if HbA1c not adequately controlled with metformin and/or empagliflozin (or if not tolerated)
- Initiate GLP-1 receptor agonist at a low dose and up-titrate slowly to reduce the risk of gastrointestinal effects
Best Practice Tip: For patients with co-morbid CKD, type 2 diabetes and heart failure, apply for funded empagliflozin under the Special Authority for heart failure and funded dulaglutide/liraglutide under the Special Authority for diabetes if the patient’s HbA1c remains above target.
N.B. More studies are needed to determine the role of GLP-1 receptor agonists in CKD management for people without diabetes; emerging evidence suggests benefit with semaglutide in those who are overweight/obese. Click here for approved indications for GLP-1 receptor agonists in New Zealand.
Non-steroidal mineralocorticoid receptor antagonists (MRAs): not routinely available
- Non-steroidal MRAs are not approved nor readily available in New Zealand, therefore, are not part of routine management
- Internationally, they are recommended for people with CKD (with an eGFR > 25 mL/min/1.73 m2) and diabetes who have persistent albuminuria (> 3 mg/mmol) despite taking the maximum tolerated dose of an ACE inhibitor/ARB
- Steroidal MRAs (e.g. spironolactone, eplerenone) are not a suitable substitute for patients in whom a non-steroidal MRA is recommended. They may be prescribed to patients with CKD and co-morbid heart failure, hyperaldosteronism or resistant hypertension; caution is required due to risk of hyperkalaemia and reversible decline in glomerular filtration.
Consider other pharmacological treatments
- Initiate a statin (atorvastatin or rosuvastatin if Special Authority criteria are met), with or without ezetimibe, in patients with an eGFR ≥ 15 mL/min/1.73 m2 and CVD risk ≥ 10% (or ≥ 5% in Māori)
- Consider a statin after discussing benefits and risks in patients with a CVD risk of 5 – 10%
- Statin treatment may benefit any patient with CKD regardless of their calculated CVD risk, e.g. those with persistent albuminuria
- Consider long-term use of low-dose aspirin for secondary prevention if established CVD
- Potentially nephrotoxic medicines (e.g. NSAIDs, lithium) may need to be switched or discontinued
Ongoing monitoring of treatment
Click here for suggested monitoring and investigation schedule.
- Review eGFR, urine ACR and blood pressure at least annually, in addition to other relevant laboratory investigations, e.g. serum electrolytes, full blood count.
- Ensure vaccinations are up to date, e.g. influenza, COVID-19, pneumococcal and meningococcal, herpes zoster (Shingrix), hepatitis A and B, Haemophilus influenzae type b
- Discuss with or refer to a nephrologist as needed, e.g. if complications of advanced CKD (e.g. metabolic acidosis) are identified





