Published: 5 July 2021 | Updated 1 July 2026 | What's changed?
1 July 2026
Updated HbA1c thresholds for diagnosing diabetes and pre-diabetes
7 March 2024 text updates based on changes in the empagliflozin datasheet/indications (now indicated in children aged ≥ 10 years)
Key practice points:
- The incidence of type 2 diabetes in younger adults and adolescents in New Zealand is increasing; people of Māori, Pacific
and South-Asian ethnicities are particularly at risk
- People with early onset type 2 diabetes have increased morbidity and mortality compared to those with a later onset
or to those of similar age with type 1 diabetes
- Preventing, or delaying, onset of type 2 diabetes is paramount to reducing the burden of diabetes complications; this
may be possible with careful management
- Test HbA1c levels in patients at high risk, regardless of their age, so that patients and their whānau/family
can be supported to make lifestyle changes before or soon after they develop diabetes
- The management of type 2 diabetes in younger people is essentially the same as for older people, i.e. lifestyle interventions
and metformin first-line, but treatments need to be more assertive, e.g. pharmacological treatment escalated sooner
- A high degree of patient and whānau/family engagement is crucial to maximise the benefits of lifestyle changes and ensure
that medicines are taken as prescribed
This is a revision of a previously published article. What’s new for this update:
- Updated data on the estimated prevalence of type 2 diabetes in those aged 25 – 39 years
- Begin CVD risk assessment, including HbA1c, at age 25 years for people with severe mental illness
- Updated recommendations on screening and management of type 2 diabetes in children and adolescents
New Zealand has a diabetes problem, fuelled in part by one of the highest rates of obesity in the world.1 Approximately
5% of the total population has type 2 diabetes; this is predicted to increase to 7% of the population by 2040 (equating
to an estimated 430,000 people with type 2 diabetes).2 The prevalence of diabetes is highest in older age groups,
reaching approximately 15 – 20% in people aged over 65 years; however, the prevalence is also increasing in younger people
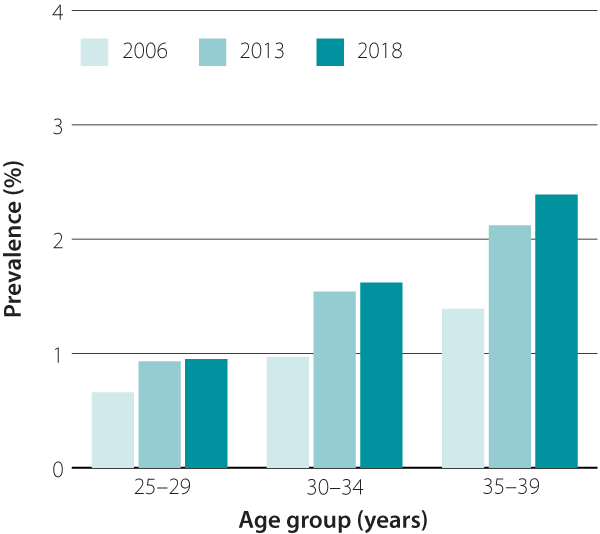
in New Zealand.3 Data from the Ministry of Health’s Virtual Diabetes Register show the prevalence of type 2 diabetes* in
people aged 30 – 39 years has nearly doubled between 2006 and 2018 (Figure 1). Increases in diagnoses
in children aged under 15 years have also been observed, although absolute numbers are still small.4 People of
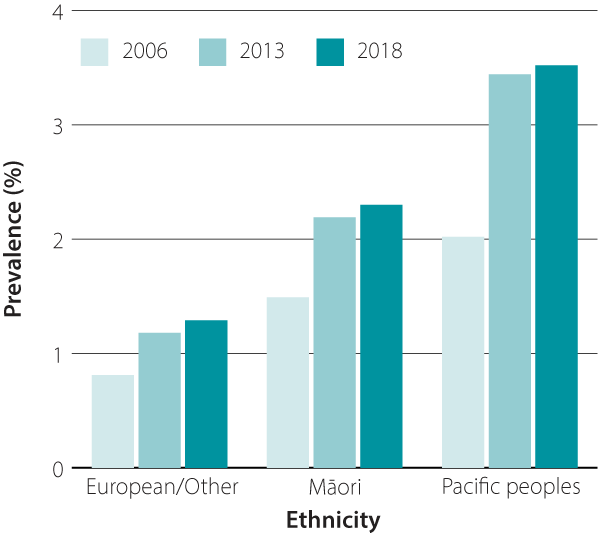
Māori, Pacific and South-Asian ethnicity, and people who are socioeconomically disadvantaged, bear a disproportionate burden
of obesity and type 2 diabetes. The prevalence of diabetes is approximately two to three times higher in adults aged 25
– 39 years of Māori and Pacific ethnicity compared to those of European ethnicity (Figure 2).
N.B. Increasing rates of type 2 diabetes may partially reflect greater awareness and testing over the years.
*The Virtual Diabetes Register does not distinguish between type 1 and type 2 diabetes. Therefore, the prevalence
of type 2 diabetes was estimated based on the assumed ratio of 90% type 2 diabetes to 10% type 1 diabetes;2 this
is a limitation when interpreting the data in younger age groups where type 1 diabetes is more prevalent.
 |
 |
|
|
| Figure 1. Changes in the estimated prevalence of type 2 diabetes from 2006 to 2018 in adults aged 25 – 39 years in New Zealand.
Source: Virtual Diabetes Register and Statistics NZ. |
Figure 2. The change in prevalence of diabetes in adults aged 25 – 39 years from 2006 to 2018, by ethnicity.
Source: Virtual Diabetes Register and Statistics NZ. |
Many young people are at high risk of developing type 2 diabetes
People with HbA1c levels of 42 – 47 mmol/mol are classified as having “pre-diabetes”, which is associated with
an increased risk of cardiovascular disease and progression to type 2 diabetes. Data from the most recent national nutrition
survey identified that 16% of the population aged under 45 years had pre-diabetes.5 It is estimated that in the
Auckland region, over 40% of people of Māori, Pacific or Indian ethnicity aged 35 – 39 years have pre-diabetes.3
Early onset results in worse health outcomes
Younger people diagnosed with type 2 diabetes, e.g. before the age of 40 years, have a higher risk of early mortality,
cardiovascular disease, chronic kidney disease and retinopathy than older adults diagnosed with type 2 diabetes or people
with type 1 diabetes at a similar age.6–8 This is largely because people diagnosed younger have diabetes for
longer and are therefore exposed to more risk, but also because glycaemic control tends to be worse and younger people are
more likely to have sporadic contact with healthcare services.6, 9
HbA1c should be tested in people at high risk of type 2 diabetes of any age to aid early detection
and therefore reduce their risk of future cardiovascular and renal complications. As type 2 diabetes is not necessarily
associated with any symptoms, patients may not even recognise that they are at risk.
Identifying people at elevated risk
Ministry of Health guidelines recommend HbA1c testing in adults (age > 18 years) with any of
the following risk factors:3
- A BMI of ≥ 27 kg/m2 for people of Māori, Pacific or South Asian ethnicities, or ≥ 30 kg/m2 for
people of other ethnicities*
- A first-degree relative who developed type 2 diabetes at an early age, e.g. < 40 years
- Long-term use of oral corticosteroids
- Females with a personal history of gestational diabetes
- Females with polycystic ovary syndrome
- Severe mental illness, particularly those on long-term antipsychotic treatment
- Known ischaemic heart, cerebrovascular or peripheral vascular disease
A specific opportunity to incorporate HbA1c testing into routine practice is the cardiovascular
risk assessment; the age at which to start assessments is now recommended as:10
- 45 years for males and 55 years for females with no known risk factors
- 30 years for males and 40 years for females of Māori, Pacific or South-Asian ethnicity
- 35 years for males and 45 years for females with known cardiovascular risk factors or at high risk of developing diabetes†
- 25 years for people with severe mental illness
*A lower BMI threshold is recommended for people of Māori, Pacific or South Asian ethnicities
due to the higher risk people of these ethnicities have of developing type 2 diabetes.3 South Asian ethnicities
include Indian, Fijian Indian, Sri Lankan, Afghani, Bangladeshi, Nepalese, Pakistani and Tibetan. People of South or East
Asian ethnicity may develop type 2 diabetes at lower BMI levels than people of European ethnicity, likely due to differences
in the accumulation of visceral fat.11
† Further information on family and personal risk factors is available at: https://www.healthnz.govt.nz/health-professionals/guidance-standards/topic/conditions/cardiovascular-disease/cardiovascular-disease-risk-assessment-and-management
Screening for type 2 diabetes in high-risk children and adolescents
Screening recommendations for type 2 diabetes in children and adolescents are guided by risk factors (Figure
3). A lower
threshold for screening is recommended for Māori and Pacific children due to the higher rates of type 2 diabetes, obesity
and CVD at younger ages in these groups.12
Diagnosis of type 2 diabetes can be based on:12
- Symptoms of diabetes or hyperglycaemic crisis and a random plasma glucose ≥ 11.1 mmol/L
- Fasting plasma glucose ≥ 7.0 mmol/L
- 2-hour plasma glucose ≥ 11.1 mmol during an OGTT
- HbA1c ≥ 48 mmol/mol
A screening frequency of two to three years is recommended, although earlier testing may be indicated in cases where there
has been excessive weight gain.12
Consider the possibility of type 1 diabetes or a monogenic form of diabetes in children or younger adults
with an elevated HbA1c without obesity, a family history or other typical features such as hypertension, dyslipidaemia
or non-alcoholic fatty liver disease. Its incidence peaks in children aged 10 – 19 years, but over half of cases are diagnosed
in people aged over 20 years.13, 14 Monogenic diabetes is estimated to be present in up to 8% of children with
features of type 2 diabetes.12
An algorithm to help clinicians diagnose monogenic diabetes has been developed by the New Zealand Society
for the Study of Diabetes: www.nzssd.org.nz/resources-and-calculators.html
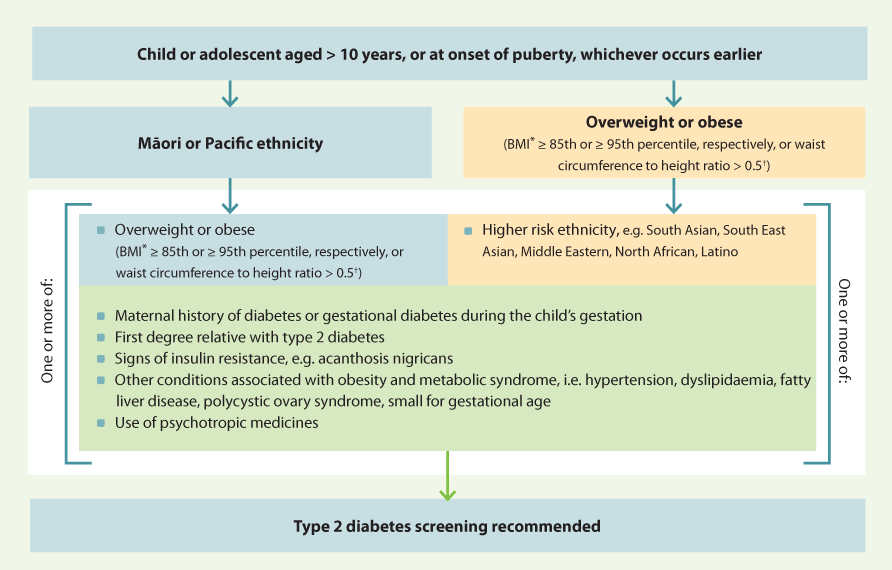
Figure 3. Type 2 diabetes screening recommendations for children and adolescents.12
* In people aged < 18 years, BMI calculations need to be adjusted for age and gender
using World Health Organization standardised guides
(see: www.who.int/toolkits/growth-reference-data-for-5to19-years)
† Calculated as waist circumference divided by height
One of the most important points to convey to people who have type 2 diabetes or pre-diabetes and their whānau/family
is that the course is modifiable. Lifestyle changes, i.e. ensuring a healthy, balanced diet and engaging in regular physical
exercise, may be difficult at first, but they can substantially improve their future health. The patient or their parent/caregiver
will have to take the lead role in making those changes, but with support from their primary care team. Setting small, incremental
goals can be helpful if patients are feeling overwhelmed by the extent of changes recommended.15
Lifestyle recommendations for adults
Weight loss has the potential to induce remission of type 2 diabetes in people who are overweight or
obese, i.e. to achieve an HbA1c < 48 mmol/mol without the use of medicines,16 and should be regarded as a core focus of treatment.
For further information on weight loss,
see: “Weight loss: the options and the evidence”
Lifestyle change in people with pre-diabetes reduces their chance of developing diabetes by approximately
50 – 60% over three years and 27% over 15 years.17, 18 This includes aiming for a 5 – 10% weight loss, 2.5 hours
per week of moderate intensity physical activity and following healthy diet recommendations.19
Referral for bariatric surgery may be appropriate for some people with a BMI between 35 – 55 kg/m2 to
assist with weight loss.15 Bariatric surgery can reduce the likelihood of developing type 2 diabetes, and in
those who already have type 2 diabetes, can induce remission, as well as reduce the risk of diabetes complications, cardiovascular
disease and some cancers.15, 20 Māori and Pacific peoples may require more support to ensure they get bariatric
surgery; fewer publicly funded bariatric surgeries are conducted for Māori or Pacific peoples than Europeans.21 Research
has shown there are higher rates of withdrawal prior to surgery in Māori and Pacific peoples.22 Discussing potential
barriers with patients can help them to prepare and plan ahead for some of the difficulties they may face if they are accepted
for surgery. Regular follow-up contact is also likely to be helpful once a patient has been accepted for surgery.
For further information on bariatric surgery, see: “Weight
loss for the prevention and treatment of type 2 diabetes”
Lifestyle recommendations for children and adolescents
Diet and weight management. Ensure that the diet is nutritionally adequate for the child or adolescent’s
growth and developmental stage.11 The goal is to prevent further weight gain in those who are overweight and
encourage weight loss in those who are obese, while maintaining normal linear growth.11
Encourage physical activity. At least 60 minutes per day of moderate to vigorous intensity exercise is
recommended for children and adolescents, with strengthening exercises included three days per week.12 Body weight
exercises and light resistance bands or weights are appropriate for children; external resistance, e.g. gym equipment, can
be added for adolescents who have reached skeletal maturity.12
Reduce recreational screen time. All children, including those with type 2 diabetes, should spend no
more than two hours per day on recreational screen time, e.g. smartphones, tablets, computers, television; approximately
four out of five children in the general population do not meet this target.12, 23
Ensure adequate sleep. Children aged 5 to 13 years should be getting 9 – 11 hours of sleep per night;
8 – 10 hours of sleep per night is recommended for adolescents aged 14 – 17 years.12 Recommend sleep hygiene
measures such as earlier and consistent bed and wake times, and reduced use of electronic media and devices at night.11
Engaging people to make changes
Identify what motivates people. Reactions to a diagnosis of type 2 diabetes, or being told they are at
high risk, can differ between people. Motivational strategies should be individualised, but a key message is that it is
never too late to “step back from the edge” and the course of type 2 diabetes is not pre-determined.
Avoid stigma and blame. Discussing lifestyle changes can be challenging, as the advice required often
carries an unspoken implication that the person has brought the disease on themselves or their child. Conveying that the
risk of type 2 diabetes and obesity is influenced by factors which are out of a person’s control, e.g. genetics, exposures
in utero or early childhood, or factors in the environment, may help alleviate some of the stigma and embarrassment associated
with obesity and type 2 diabetes. Advice on language which can help avoid blame when discussing type 2 diabetes is provided
in Table 1.
Regular follow-up is essential. Develop an agreed plan that can be used to track progress, e.g. appointment
with a practice nurse, providing advice or support via telephone or text message. A randomised controlled trial in the United
States found that participants who had completed a lifestyle intervention were less likely to regain weight if they had
telephone follow up rather than written education alone.24 Encourage patients to make one change at a time with
subsequent goals added at follow-up appointments; focus on the changes that will bring the greatest benefit, e.g. weight
loss or smoking cessation.
Connect patients to services that can assist with lifestyle changes, including referring patients to
a dietitian, providing them with a Green Prescription, or referring to programmes offered by a local PHO, DHB or Māori health
provider.
Table 1: Using language which can help avoid blame when discussing diabetes. Adapted from the American Association of Diabetes
Educators and American Diabetes Association.29
| Language/tone of conversation which may have negative connotations |
Suggestions for replacement concepts and phrases |
Things to consider |
Compliance/adherence
e.g. “You must take metformin twice a day” |
Concepts such as engagement, participation, involvement
Explain the benefits of medicine use and encourage patients to follow dosing instructions, e.g.: “Taking metformin
twice a day will make it easier for you to reduce your HbA1c level than taking it less often” |
Focus on using factual statements to emphasise how the person’s health could improve by following the advice |
Regimen/rules
e.g. “You need to do 30 minutes of moderate intensity exercise per day” |
e.g. “You’re doing around 15 minutes per day of walking. This is great - do you think you could now do a bit more?
Are there other types of exercise you would like to try? What are some of the things that might stop you from doing
more?” |
Encourage people to identify changes they want to make and help them to achieve those goals, rather than dictating
what those changes should be and judging their progress based on what you think they should achieve |
Control:
e.g. “Your diabetes is not well-controlled” |
Instead of referring to “good/bad control” explain what HbA1c level is being aimed for and the effects
of the current approach to treatment:
e.g. “Your HbA1c level is 70 mmol/mol. That is an improvement, but how about we make another goal to try
to get it even lower.”
“We started metformin last time, but it is not bringing down your HbA1c levels enough. We might need to
increase the dose.” |
Control may be impossible to achieve given the body’s systems for regulating glucose levels are failing. Try to
focus on the underlying physiology and what a patient is doing well. |
Can’t/shouldn’t/don’t
e.g. “Don’t have fizzy drinks” |
“Have you tried...”
“Would you consider....”
“I’ve found what has worked for other people is...”
e.g. encourage alternatives, such as “try water with a slice of lemon” |
This type of statement (can’t/shouldn’t/don’t) can make people feel they are being given orders |
Lacking motivation or unwilling to engage
e.g. “So you are not willing to start insulin?” |
Focus on perceived barriers and why a patient doesn’t want to proceed with a plan of action. This may lead to
potential solutions.
e.g. “From what you are saying, your main concerns around starting insulin are weight gain and the potential embarrassment
of injecting yourself at work?” |
Most people want to live a healthy life. The challenge with managing diabetes and weight is that people can feel
there are barriers stopping them from changing, or may not appreciate the benefits of doing things differently. People
may feel it is not worth the effort or is unachievable. |
The approach to pharmacological management of type 2 diabetes in patients with early onset is essentially the same as
for any patients with type 2 diabetes, i.e. metformin first-line, followed by other oral and injectable glucose-lowering
medicines, as appropriate (also see: “Managing type 2 diabetes in children and adolescents”). However, faster escalation
of treatments may be required and lower targets for glycaemic control are justified.25 Patients with early onset
type 2 diabetes can have a more rapid increase in HbA1c levels, despite treatment, and are likely to require
more frequent dose increases, use of multiple oral medicines or earlier addition of insulin than older patients with type
2 diabetes.26 Effective communication and engagement with patients and their whānau/family in regards to the
importance of adhering to their prescribed medicines is of particular importance in this age group. Reinforce that if they
can gain control with assertive treatment and lifestyle, it may be possible to dial treatment back over time.
For further information on setting a HbA1c target and prescribing glucose-lowering medicines for
patients with type 2 diabetes, see: "Type 2 diabetes management
toolbox: from lifestyle to insulin"
For further information on initiating insulin, see: "Initiating insulin
for people with type 2 diabetes"
Metformin for patients with “pre-diabetes”
Metformin can be prescribed (unapproved indication) to reduce the risk of developing type 2 diabetes in patients at high
risk (e.g. HbA1c of 42 – 47 mmol/mol), but should be considered an adjunct treatment in addition to changes in
diet and activity levels.17 Metformin reduces the risk of developing type 2 diabetes by approximately one-third
after three years, and approximately 20% after ten years, compared to a placebo medicine in patients at high risk.27
Managing type 2 diabetes in children and adolescents
Children and adolescents with type 2 diabetes are typically managed in secondary care, with primary care providing additional
support to the patient and their whānau/family. A HbA1c target of < 48 mmol/mol is recommended for children
and adolescents to reduce the long-term risk of developing diabetes complications.12 Metformin is the first-line
pharmacological treatment, up to a maximum dose of 2 g, daily.12 If the patient’s HbA1clevel is ≥
69 mmol/mol or they are symptomatic at diagnosis, insulin is initiated in addition to metformin. Once HbA1c levels
have reduced to target, insulin can be titrated down and withdrawn.12
Previously, metformin and insulin were the only medicines approved in New Zealand for use in people with type 2 diabetes
aged < 18 years.12 Since November, 2023, empagliflozin is now indicated in children aged ≥ 10 years as monotherapy if metformin is not tolerated (and diet and exercise alone do not provide adequate glycaemic control), or in combination with other glucose-lowering medicines (under specialist supervision) if glycaemic control remains poor. Other glucose-lowering medicines approved for use in adults only, e.g. dulaglutide,
vildagliptin, sulfonylureas and pioglitazone, may be considered for children and adolescents with type 2 diabetes, on the
recommendation of a paediatric endocrinologist.12
Despite being young, people diagnosed with diabetes at an early age may already have complications and should have their
retinal, foot, renal and cardiovascular health fully assessed and managed at diagnosis. Also consider associated co-morbidities,
such as sleep apnoea or non-alcoholic fatty liver disease.
Managing cardiovascular and renal risk
Cardiovascular and renal diseases are the main causes of early mortality in people with type 2 diabetes, and preventing
the onset or progression of these conditions in young people should be a focus of management.28 Lifestyle changes
can improve markers of cardiovascular risk, such as blood pressure and lipid levels, however, pharmacological treatment
should be initiated if lifestyle changes result in insufficient improvements, or if the patient’s CVD risk is high.
For further information on managing cardiovascular and renal risk in patients with
type 2 diabetes, see: https://www.healthnz.govt.nz/health-professionals/guidance-standards/topic/conditions/cardiovascular-disease/cardiovascular-disease-risk-assessment-and-management
An online calculator for determining the risk of cardiovascular and renal disease in patients with type 2
diabetes is available at: www.nzssd.org.nz/cvd_renal/
Transition stages are a risk time for worsening diabetes management
Guidelines recommend that all adolescents with type 2 diabetes transition to an adult diabetes service.12 This
transition period can be a time when issues with appointment attendance, adherence to medicines and lifestyle interventions,
worsening glycaemic control, acute and chronic complications arise.12 Primary care should establish who is responsible
for the patient’s diabetes care and ensure that they are regularly followed up, including reviews of their glycaemic control,
medicines regimen, mental health and wellbeing, and undergo a diabetes review annually.
For further information on the annual diabetes review, see: “The
annual diabetes review: screening, monitoring and managing complications”





