
B-QuiCK: Migraine
Diagnosis
Migraine is characterised by recurrent episodes of moderate-to-severe headache (typically lasting four hours or longer) along with other symptoms, e.g. nausea, vomiting, photophobia, phonophobia, aggravation by physical activity
- Take a symptom history - ask about:
- Pain characteristics, e.g. location, pattern and severity
- Frequency and duration
- Associated symptoms
- Aggravating factors
- Impact on activities
Click here for differentiating features between migraine and other primary headaches
- Exclude serious secondary causes of headache;
 click here for red flags. Conduct detailed physical examination and request other investigations as required.
click here for red flags. Conduct detailed physical examination and request other investigations as required.
- Ask the patient to complete a headache diary: record triggers, frequency and severity, analgesic use and impact on daily activities over time
- This supports a diagnosis of migraine and provides a baseline for monitoring treatment response
Migraine is formally diagnosed according to ICHD-3 criteria – patients must have experienced at least five headache episodes in their lifetime with the following characteristics:
At least two of:
- Unilateral
- Throbbing or pulsating
- Moderate-to-severe pain
- Aggravated by, or causing avoidance of, routine physical activity
|
AND |
One or both of:
- Light sensitivity and sound sensitivity
- Nausea and/or vomiting
|
AND |
Duration lasting 4 – 72 hours |
“Migraine with aura” can be diagnosed if there have been at least two episodes of fully reversible visual, sensory, speech/language, motor, brainstem and/or retinal aura symptoms, with multiple specific aura symptom characteristics.
Management
Goal: reduce migraine frequency and severity to improve quality of life
Validated tools, e.g. Migraine Disability Assessment (MIDAS), help quantify impact on quality of life
- Set realistic treatment expectations early; migraine is a neurological condition that cannot be cured, but can be managed to be tolerable
- Encourage positive lifestyle changes, e.g. getting adequate rest, regular meals, avoiding known triggers, regular exercise
- Trial non-pharmacological strategies, e.g. relaxation and coping techniques, CBT
- Some evidence for complementary treatments, e.g. greater occipital nerve blocks, acupuncture, neuromodulation devices
- Supplements not routinely recommended but some evidence for magnesium, riboflavin (vitamin B2), coenzyme Q10 and feverfew extract
- No compelling evidence for other interventions such as tinted glasses, daith or tragus piercings, but support patients in trialling if theoretical benefit and unlikely to harm
- Consider referral to other primary care team members (e.g. health improvement practitioner) or healthcare professionals (e.g. physiotherapist) as needed
Acute migraine treatment
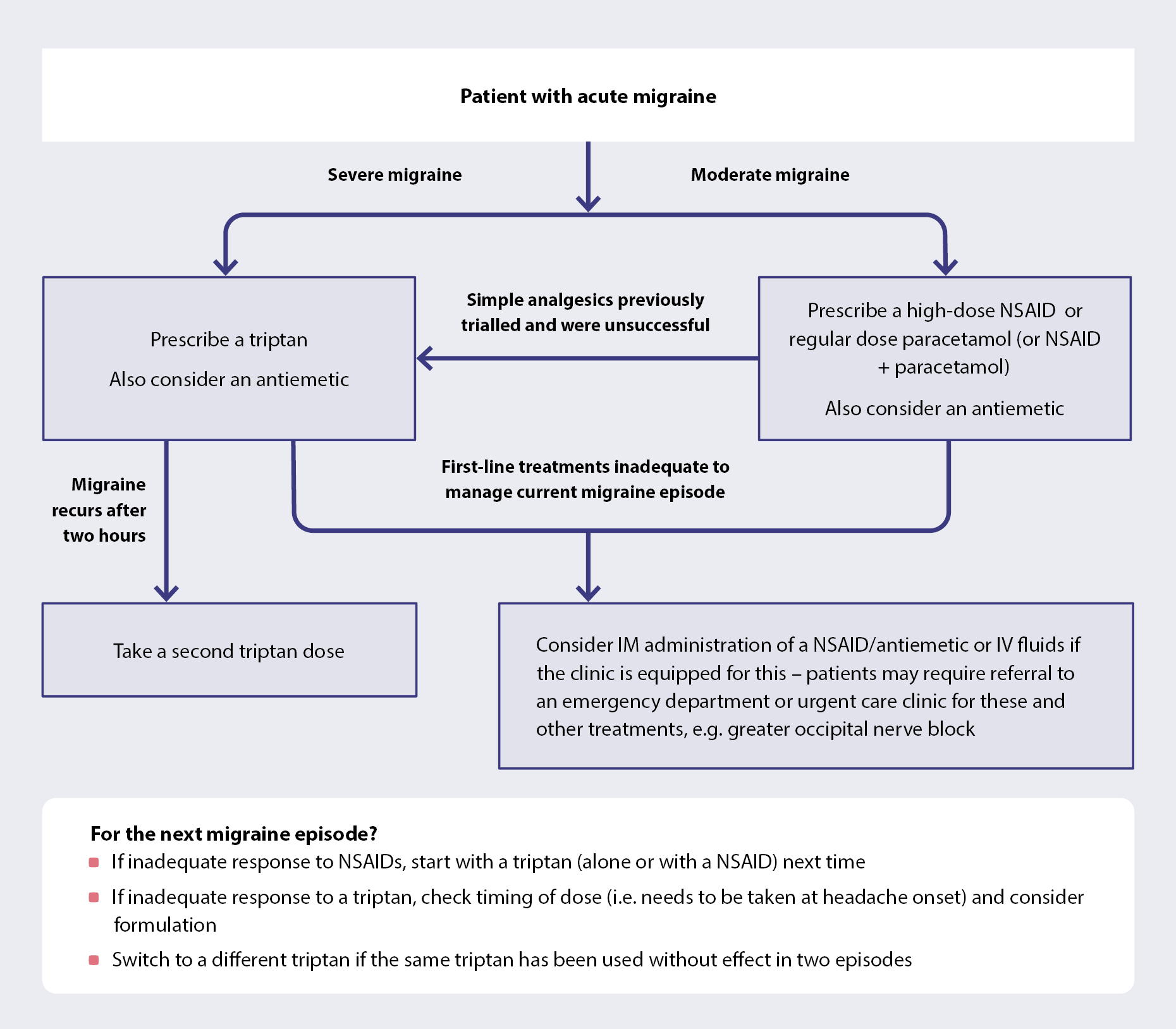
Click here for dosing of medicines for acute migraine
- Start acute migraine treatment as soon as possible after headache onset; goal is to be pain free within two hours
- Limit analgesics to < 15 days/month and triptans to < 10 days/month to reduce medicine overuse headache risk
Migraine prophylaxis
Migraine prophylaxis is indicated if:
- ≥ 4 migraine episodes or ≥ 8 headache days per month (use clinical judgement, e.g. patient with fewer but severe episodes may benefit from prophylaxis)
- Acute treatments are ineffective, not tolerated/contraindicated or overused
No single approach to migraine prevention is effective for every patient. Select a medicine based on co-morbidities, risk factors, medicine interactions, prior treatment history, patient preference and cost.
Main funded options: beta blockers (e.g. propranolol, metoprolol), antidepressants (e.g. amitriptyline), candesartan, sodium valproate and topiramate. Click here for an overview of funded medicines for migraine prophylaxis.
- Generally less effective than CGRP-targeted treatments (see below), but many patients can still achieve satisfactory control with these options
Non-funded options: CGRP monoclonal antibodies (SC injection), e.g. fremanezumab, galcanezumab, erenumab, small-molecule CGRP receptor antagonists, e.g. atogepant (oral), and Botox (injection; chronic migraine)
- CGRP-targeted treatments are generally more effective and better tolerated than conventional migraine preventatives. Base selection on patient preference for route of administration, dosing frequency and cost.
Trial preventative medicines for two to three months at the maximum tolerated dose (or three to six months for CGRP-targeted treatments) before assessing response; improvement may be gradual
- 30 – 50% reduction in migraine frequency and severity is an adequate response, or less if patients experience other benefits, e.g. improved quality of life, functional ability
Assess treatment response and review ongoing need for prophylaxis
- Follow up regularly while the dose is up-titrated, and then can reduce frequency of follow-up over time
- Assess adherence, adverse effects, change in migraine frequency and severity and quality of life (based on headache diary), and reinforce lifestyle measures
- Consider switching to an alternative medicine or trialling combination treatment if inadequate response after three to six months
- Consider co-morbidities, medicines mechanism of action and interactions when prescribing combination treatment
- Discuss with, or refer to, a neurologist if inadequate response to multiple migraine preventatives
- Review need for ongoing use after 6 – 12 months of effective treatment; use clinical judgement and consider patient’s goals of treatment and preferences when determining optimal time to withdraw
- Gradually withdraw treatment in a step-wise manner
- Migraine frequency may worsen during withdrawal (particularly with CGRP-targeted treatments); temporarily increase dose or re-start medicine (if threshold for prophylaxis is met again)
- Ensure acute treatments are available to bridge any episodes





