Published: 28th April, 2026
Key practice points
- Migraine is a complex neurological condition characterised by recurrent episodes of moderate-to-severe headache that typically lasts at least four hours along with other symptoms such as nausea, vomiting, photophobia, phonophobia or aggravation by physical activity
- Migraine is associated with a significant impact on quality of life and disability
- The diagnostic work-up of a patient with suspected migraine begins with taking a symptom history, followed by physical examination as indicated to exclude secondary causes of headache. Formal diagnosis is made according to criteria in the International Classification of Headache Disorders (ICHD-3).
- A headache diary (reporting triggers, symptom frequency and severity, analgesic use, impact) can support a diagnosis of migraine and provide a baseline for monitoring response to treatment
- Initial treatment during an acute migraine episode with an oral NSAID (or NSAID and paracetamol) is usually appropriate for most patients. Treatment can be stepped up to include a triptan for the next episode if simple analgesics were not effective or a triptan can be started initially in patients with severe symptoms. Combination treatment may be required.
- An antiemetic, e.g. metoclopramide, can be added regardless of whether the patient experiences nausea/vomiting as they can also enhance gastrointestinal absorption of other medicines
- Setting realistic goals and patient expectations are key components of migraine management: migraine is a neurological condition that cannot be cured, but it can be managed to an extent that is tolerable in many cases
- Encourage patients to make lifestyle changes that could be contributing to migraine (e.g. getting adequate rest, regular meals, avoiding known triggers, regular exercise), and trial non-pharmacological treatment strategies, e.g. relaxation and coping techniques
- Consider migraine prophylaxis for patients who experience multiple episodes per month (≥ 4 migraine episodes or ≥ 8 headache days), or if acute treatments are ineffective, not tolerated/contraindicated or overused
- Trial for two to three months at the maximum tolerated dose before assessing response
- Review the need for ongoing use after 6 – 12 months of effective treatment
- The choice of migraine preventative medicine largely depends on patient co-morbidities. The main funded options include beta blockers (e.g. propranolol, metoprolol), antidepressants (e.g. amitriptyline), candesartan, sodium valproate and topiramate.
- Non-funded options for migraine prophylaxis are also available, such as calcitonin gene-related peptide targeted treatments (e.g. fremanezumab, atogepant). These medicines are effective and are generally better tolerated than conventional migraine prophylaxis medicines, but cost may limit access.
Migraine is a complex life-long neurological condition characterised by recurrent episodes (“attacks”) of moderate-to-severe headache typically lasting for 4 – 72 hours, along with other symptoms such as nausea, vomiting, photophobia, phonophobia or aggravation by physical activity.1, 2 To be formally diagnosed with migraine, a person must have experienced at least five headache episodes characteristic of migraine in their lifetime (see: “Diagnose migraine based on ICHD-3 criteria”).3 People with migraine experience a median frequency of two episodes per month, but this varies widely.2 Migraine is associated with a significant impact on quality of life, including employment, education, sleep, relationships and mental health, and it is a predominant cause of disability worldwide (see: “Migraine: From a patient perspective”).4, 5
Migraine is estimated to affect 15% of people in New Zealand, consistent with the global prevalence.4, 6 Migraine is more prevalent among some populations, e.g. in the 2023/24 New Zealand Health Survey, 19% of Māori adults and 24% of adults with a disability reported migraine symptoms in the last three months.6 Migraine is commonly under-diagnosed and consequently under-treated;7 half of respondents in the Health Survey who reported migraine symptoms in the last three months, had not been formally diagnosed (see: “Barriers to migraine diagnosis and management”).6
Migraine can occur at any age but typically begins in puberty and adolescence.1 The prevalence of migraine peaks between ages 30 – 40 years,2, 8 and tends to decline with age. It is unusual for new-onset migraine to occur in people after age 50 – 60 years.1, 8 Females are twice as likely as males to experience symptoms of migraine.6, 9
Migraine presentation in children can be different to adolescents and adults, e.g. abdominal migraine, benign paroxysmal vertigo and benign paroxysmal torticollis may occur.3 For further information, click here.
Migraine phases and classifications
Classically, there are four phases to migraine, however, not all people with migraine progress through these phases:1, 10
- Prodrome – symptoms such as yawning, fatigue and stiff neck can occur hours to days prior to headache onset
- Aura – characterised by transient visual, sensory or speech symptoms, that typically evolve over minutes and usually last up to one hour. Aura occurs in approximately one-third of people who experience migraine; usually an aura precedes headache, but it can occur during or after.2, 11
- Headache – typically lasts for 4 – 72 hours and is associated with other symptoms, e.g. nausea, photophobia. The headache is characteristically unilateral (but it can be bilateral) and pulsating, throbbing and moderate to severe in nature.
- Postdrome – symptoms such as tiredness, poor concentration and mood changes can persist for up to two days following headache resolution
Migraine can be classified as either episodic (most common) or chronic.1, 3 Chronic migraine is when a patient experiences 15 or more headache days per month, of which at least eight days have features of migraine, for at least three months.3 It is possible for people to switch between classifications over time.1, 12 Chronic migraine typically evolves from episodic migraine due to increasing frequency of episodes, factors related to the management of migraine, e.g. inadequate treatment of acute episodes, medicine overuse, or other co-morbidities, e.g. obesity, depression.1, 13 People with chronic migraine tend to experience greater disability and impact on quality of life, and may require additional supports and migraine prophylaxis introduced at an earlier stage.2, 12
Migraine pathogenesis is multifactorial
The pathogenesis of migraine is multifactorial and not completely understood. It is believed that a combination of genetic and environmental factors, as well as activation of the trigeminovascular pathway of the brain and release of neuropeptides, e.g. calcitonin gene-related peptide (CGRP), are involved.1, 14 CGRP is involved in a range of actions, including vasodilation, pain transmission and inflammation.15, 16 Some people report experiencing migraine triggers, such as dehydration, excess caffeine, alcohol, poor sleep, bright lights, change in weather, odours or hormone fluctuations.17, 18 In some cases, the presumed trigger may be an early sign of migraine onset, e.g. bright lights may be a consequence of the patient experiencing photophobia during a migraine, rather than triggering the episode.1
Risk factors and co-morbidities associated with migraine include family history and genetics, metabolic conditions (e.g. obesity), cardiovascular disease, psychological factors (e.g. stress, depression, anxiety) and sleep disorders.1, 19, 20 Females are more likely to experience migraine due to fluctuating hormone levels associated with the menstrual cycle (see: “A focus on menstrual migraine”).6, 9
It feels very lonely. No one understands what I've been dealing with 24/7 for the last 5 years. My migraine has literally never stopped, even for a moment, since it took hold out of the blue… I do not have distinct attacks, triggers or things I can do to alleviate it. Trying to explain that to people is hard…. People think a migraine is just a headache, take some Panadol and carry on. The way I try to describe it to people is that it's like being incredibly hungover, on a boat which is broken down out at sea. But the hangover is not going away as the day progresses or after eating food or after some sleep. The hangover is there today, tomorrow, it will still be there next week, next month, probably next year and the boat I'm stuck on, is broken and seemingly never coming back to shore. 35 – 44 years Male NZ European/Other)
35 – 44 years Male NZ European/Other)
– Unpublished quote from the 2022 Migraine in Aotearoa Survey
Barriers to migraine diagnosis and management
Barriers to seeking care for migraine have been surveyed among a group of over 500 people with migraine in New Zealand (2022), and a small group of primary care clinicians (2024).7, 21
Reported barriers included:7, 21
- Lack of patient awareness or understanding of migraine and its treatment
- Stigma. Some patients felt judged or misunderstood by healthcare professionals (e.g. symptoms not given appropriate attention or attributed to mental health issues), by employers (e.g. difficulty in taking sick leave) or by family/whānau and friends (e.g. by cancelling plans, unable to do housework). Primary care clinicians also reported a lack of societal understanding of the potential severity of migraine, as well as stigma of a chronic invisible condition.
- Availability of primary and secondary care services, e.g. inability to register with primary care, limited access to specialist care, e.g. neurologist, via the public healthcare system
- There are significant shortages in the New Zealand neurology workforce; a 2024 analysis reported approximately one neurologist per 63,000 population (1/72,000 population for adult public and private hospital services; 1/75,000 population for adult public hospital services)22
- Long wait times for appointments
- Cost related to appointments, e.g. consultation fees, costs of transport to appointments, and non-funded treatments
Patients also felt that healthcare professionals could improve their knowledge about migraine and its management, and have better communication with patients regarding care plans.21
The diagnostic work-up of a patient with suspected migraine begins with taking a focused symptom history, followed by a physical examination and other investigations as needed to exclude secondary causes of headache (see: “Exclude serious secondary causes of headache”).2, 20
Take a focused symptom history
A symptom history to determine the presence of characteristic features is key to diagnosing a patient with migraine; headache is only one symptom of migraine.2 To distinguish migraine from other primary headaches (e.g. cluster, tension), ask the patient about:1, 2, 8, 11, 20
- Pain characteristics, e.g. location, pattern and severity
- Migraine is characterised by intense moderate-to-severe headaches that are typically pulsating in nature. Pain is classically unilateral, but can also be bilateral.
- In contrast, tension headaches are bilateral and described as pressing/tightening in nature and of mild or moderate intensity. Cluster headaches are unilateral and vary in nature, e.g. can be sharp, burning, throbbing, tightening, and of severe or very severe intensity.
- Frequency and duration
- One to two migraine episodes typically occur per month, but this varies. Episodes usually last for 4 – 72 hours.
- In contrast, tension headache can last hours to days and cluster headaches last from 15 minutes to three hours. The frequency of cluster headaches is usually one to three episodes per day, for two to three months.
- Associated symptoms
- Migraine is associated with other symptoms in addition to headache, e.g. aura, nausea, vomiting, dizziness, fatigue, poor concentration, photophobia, phonophobia, neck pain
- In contrast, these symptoms are not usually present with tension headache. In cluster headache, there may be conjunctival injection, lacrimation, nasal congestion, rhinorrhoea and eyelid swelling/drooping on the same side as the headache.
- Aggravating factors
- Migraine is often aggravated by, or causes avoidance of, routine physical activity
- In contrast, symptoms are not aggravated by routine physical activity with tension or cluster headaches
- Impact on activities
- Migraine impacts multiple aspects of daily life, e.g. work, education, relationships
- Tension and cluster headache can also affect daily activities
Ask about previously trialled treatments
Determine what treatments the patient has trialled in the past to manage headache or other associated symptoms, e.g. non-pharmacological strategies, prescription, over the counter, complementary and alternative medicines, and dose(s), and how effective they were.8, 9
A headache diary can support a diagnosis of migraine
Asking the patient to complete a headache diary over time, recording frequency, severity, impact on daily activities, triggers and analgesic use, can help support a diagnosis of migraine.9, 11 It will also provide a baseline for monitoring future response to treatment.2
An example of a template for a headache diary is available from: https://healthify.nz/tools/h/headache-diary. Apps are also available for patients to record details of their headaches: https://healthify.nz/apps/m/migraine-and-headache-apps.
Exclude serious secondary causes of headache
There are a variety of secondary causes of headache that are important to rule out, e.g. subdural haematoma, intracranial tumour, giant cell arteritis.15, 20 If a secondary cause is suspected (see box), conduct a more detailed examination as required, e.g. focused neurological examination (including fundoscopy), assessment of the head (including temporal arteries for prominence, erythema and tenderness) and neck for general or discrete tenderness, stiffness or limitations in the range of movement.2, 8 Discuss with, or refer the patient to, a relevant specialist as needed. Referral for imaging, e.g. CT head scan, is not routinely required, but it may be considered in select cases; view referral criteria here.
 Red flags requiring further action
Red flags requiring further action
The SNOOP4 mnemonic is commonly used to guide clinicians in identifying red flags associated with headache:2, 11, 23
- Systemic symptoms (e.g. fever, chills, myalgia, night sweats) or condition (e.g. history of malignancy, HIV infection, immunosuppression)
- Neurological symptoms or signs, e.g. confusion, diplopia, neurological deficit
- Onset – sudden onset headache reaching maximum intensity within minutes (thunderclap headache)
- Older age – onset after age 50 years
- Progressive headache – change in headache features, pattern or severity over days or weeks
- Precipitated by Valsalva, cough or sneeze
- Postural or exertional aggravation, e.g. headache worsened or triggered by standing, lying down or exercise
- Papilloedema
Diagnose migraine based on ICHD-3 criteria
To meet International Classification of Headache Disorders (ICHD-3) criteria for the formal diagnosis of migraine (“migraine without aura”), patients must have experienced at least five headache episodes in their lifetime with the following characteristics:3
At least two of:
- Unilateral
- Throbbing or pulsating
- Moderate-to-severe pain
- Aggravated by, or causing avoidance of, routine physical activity
|
AND |
One or both of:
- Light sensitivity and sound sensitivity
- Nausea and/or vomiting
|
AND |
Duration lasting 4 – 72 hours |
For formal diagnosis of “migraine with aura”, at least two episodes that include fully reversible visual, sensory, speech/language, motor, brainstem and/or retinal aura symptoms as well as the presence of multiple specific aura symptom characteristics are required.3 In rare cases, subtypes of migraine with aura can occur, including migraine with brainstem aura, hemiplegic migraine and retinal migraine.3 See ICHD-3 for formal diagnostic criteria of migraine with aura and subtypes.
The main goal of migraine management is to improve the patient’s quality of life by reducing the frequency and severity of episodes.15 This is achieved through a combination of lifestyle changes and non-pharmacological treatment strategies, appropriate management of co-morbidities that can influence migraine, e.g. anxiety, as well as acute and preventative migraine medicines, as needed.9, 24 It is important to validate the impact that migraine has on the patient and set realistic treatment expectations early; migraine is a neurological condition that cannot be cured, but it can be managed to an extent that is tolerable in many cases.2, 20
Determine impact on the patient’s quality of life
Once a patient has been diagnosed with migraine, determine the impact that it has on their quality of life, including education/employment, household tasks, social and family life.8, 9 Validated tools, such as Migraine Disability Assessment (MIDAS) can be used to help quantify the level of disability.5, 18 This may also assist in identifying additional support required from the wider primary care team, e.g. health improvement practitioner, and provides a baseline for monitoring response to treatment.
I would give anything to have a semi small amount of a normal life. (35 – 44 years Female NZ European/Other)
– Unpublished quote from the 2022 Migraine in Aotearoa Survey
Lifestyle changes and non-pharmacological options may be effective
Lifestyle factors that may reduce the frequency of migraine include:9, 17
- Aerobic exercise
- Sufficient sleep
- Good hydration and limiting caffeine intake, e.g. up to two coffees per day25
- Regular meals
Patients should generally be encouraged to avoid known migraine triggers, but it is important to balance this against the potential for this behaviour to be restrictive and inadvertently increase anxiety and impact quality of life.5, 9 Reducing stress through coping strategies, relaxation techniques, e.g. mindfulness, and cognitive behavioural therapy (CBT) can be helpful for many patients with migraine.2, 9, 17 There is also some evidence (low quality) for other complementary treatments, such as acupuncture, neuromodulation devices (e.g. supra-orbital transcutaneous electric nerve stimulator) and greater occipital nerve blocks (see: “Greater occipital nerve blocks for migraine”).18, 26 However, access to these treatments in New Zealand is often limited due to cost.
Consider whether the patient may need appointments with other members of the primary care team who can offer different types of support and treatment, e.g. health improvement practitioner to help patients with making lifestyle changes or managing anxiety.7 Referral to a physiotherapist may provide temporary relief for patients with a musculoskeletal component to migraine, e.g. neck pain.7
Free online CBT courses are available from Just a Thought on a range of topics, including anxiety, depression and coping with stress. CBT apps are also available.
Other options for migraine prevention: limited evidence of effectiveness
There are a wide variety of reported interventions that people with migraine may wish to trial, e.g. tinted glasses, daith or tragus piercings.12 There is no compelling evidence that any of these interventions prevent migraine,12 but patients should be supported to trial an intervention if it could theoretically provide some benefit and is unlikely to cause harm.
Supplements are not routinely recommended for migraine prevention due to limited evidence overall.8, 24 However, there are certain supplements that do have some evidence in migraine that should be chosen if a patient wishes to trial alternative treatments, e.g. magnesium, riboflavin (vitamin B2), coenzyme Q10 and feverfew extract.12, 16
Greater occipital nerve blocks for migraine
A greater occipital nerve block is an injection of local anaesthetic (with or without a corticosteroid) into the occipital nerves at the base of the skull. There is some evidence that greater occipital nerve blocks may reduce the severity and frequency of migraine episodes in the short term (weeks to months).2, 23, 27 The procedure is generally well tolerated; injection site pain, vertigo and nausea are common adverse effects.23, 27
Some primary care clinicians are skilled in this procedure and can offer this treatment in the community, however, in most cases, patients will access greater occipital nerve blocks via secondary care neurology or pain services or private clinics. They may also be administered in an acute setting, e.g. emergency department, for patients during a severe episode that has not responded to other acute treatments.23
The pharmacological treatment of patients with acute migraine can occur in either a stepped or stratified approach (see Figure 1 for an acute treatment overview):2, 9
- Stepped – begin with simple analgesics, followed by oral triptans for the next episode in those with an inadequate response, or a combination of the two
- In many cases, patients will already have trialled simple analgesics prior to presenting to general practice; ask about what medicines and doses have been taken, frequency of use and effectiveness.8, 15 Prior to stepping up treatment to a triptan, consider prescribing a higher dose or an alternative NSAID to what the patient has previously trialled.8, 15
- Stratified – target treatment according to migraine severity, e.g. begin with a triptan in patients with severe migraine
An antiemetic will also be needed for many patients with migraine, as nausea/vomiting is common, and an antiemetic can also help to improve efficacy of analgesics (see: “Consider prescribing an antiemetic”).2
Acute migraine treatment should be started in patients as soon as possible after headache onset: the goal is to be pain free within two hours.2, 9, 24 To manage the patient’s current migraine episode if they have an inadequate response to first-line treatments, consider intramuscular (IM) administration of a NSAID/antiemetic or intravenous (IV) fluids if the clinic is equipped for this. Alternatively, patients may require referral to an emergency department or urgent care clinic for these and other treatments, e.g. greater occipital nerve block.
Switching to an alternative acute treatment or combination treatment for the next migraine episode is likely to be required for patients with inadequate response with their current regimen.2, 28 To help guide whether a patient’s current acute migraine treatment plan is effective, the Migraine Treatment Optimization Questionnaire-4 can be used; a low score indicates that treatment may need to be altered.18, 20
When prescribing acute migraine treatments, advise patients about the possibility of developing medicine overuse headache.2, 9 To reduce this risk, analgesics and triptans should be taken for no more than 10 – 15 days per month.2, 9, 24 A headache diary can help patients keep track of their analgesic use, and guide when migraine prophylaxis is indicated (see: “The prophylaxis of migraine”).
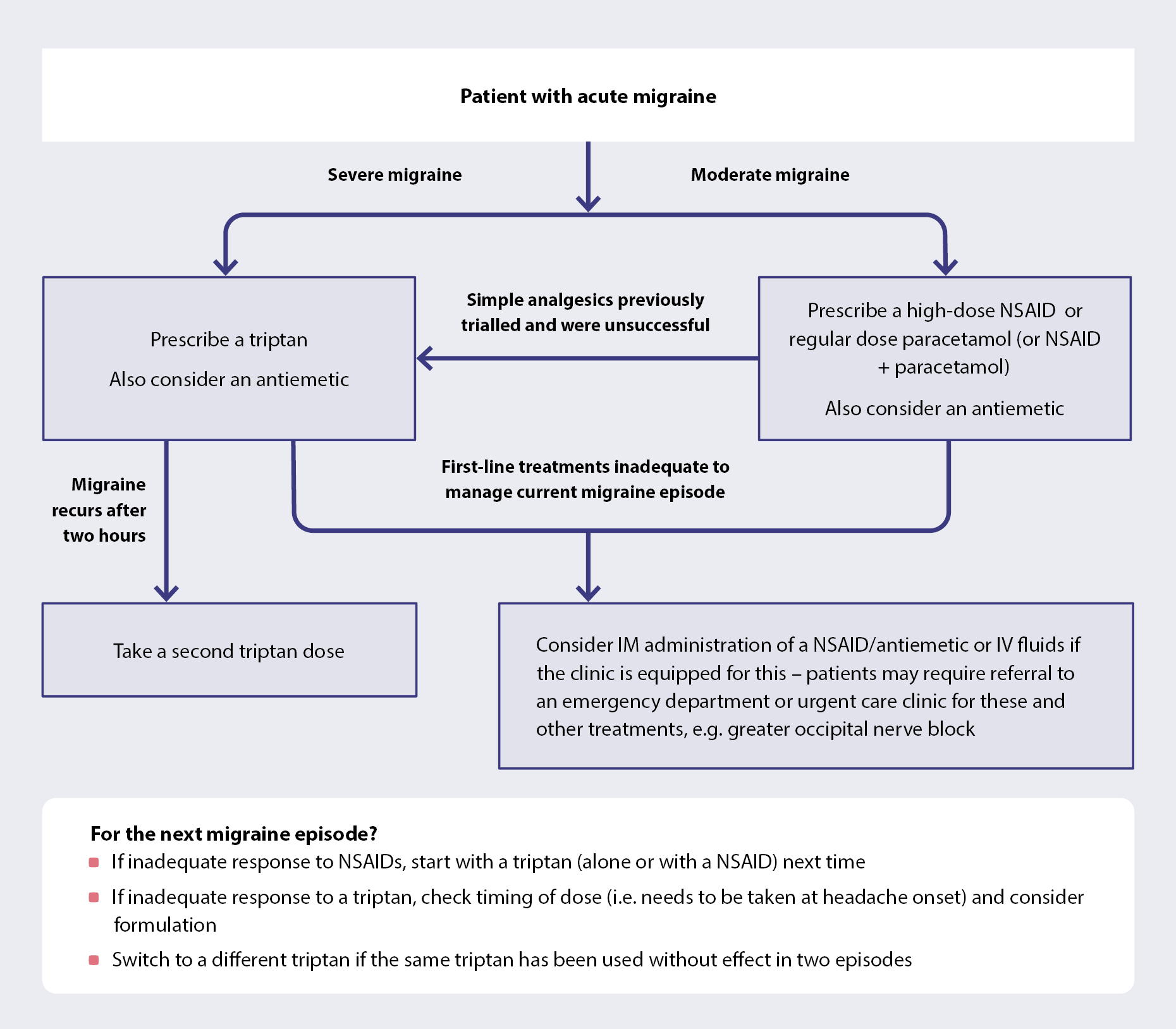
Figure 1. An overview of acute migraine treatment.2, 9, 28
Simple analgesics are usually first line
A high-dose NSAID (e.g. ibuprofen, naproxen, diclofenac, aspirin) is usually first line for patients with acute migraine (Table 1);2, 9 alone or in combination with paracetamol. Paracetamol alone is generally less effective, but is an option for patients who are pregnant or breast-feeding (see: “Migraine during pregnancy and breast-feeding”), or patients who cannot take NSAIDs due to medicine interactions or gastrointestinal co-morbidities.9, 20 Opioids are not recommended for the treatment of migraine.2, 11
Different NSAIDs are considered similarly effective for acute migraine; choice is based on individual patient factors, e.g. non-oral formulations, such as a diclofenac suppository or IM injection, may be preferable for patients with nausea/vomiting.15, 29 To reduce the risk of medicine overuse headache, use of analgesics should be limited to fewer than 15 days per month.24
Table 1. Medicines for acute migraine.2, 9, 30
| Medicine |
Usual dose for migraine |
Maximum dose per day |
| Simple analgesics |
| Ibuprofen |
400 – 600 mg |
2,400 mg |
| Naproxen |
250 – 500 mg |
1,000 mg |
| Diclofenac |
50 – 100 mg |
150 mg |
| Aspirin |
900 – 1,000 mg |
4,000 mg |
| Paracetamol* |
1,000 mg |
4,000 mg |
| Triptans |
| Rizatriptan |
10 mg |
30 mg |
| Sumatriptan |
50 – 100 mg (oral)
6 mg (subcutaneous) |
300 mg (oral)
12 mg (subcutaneous) |
| Antiemetics |
| Metoclopramide |
10 mg |
30 mg |
| Prochlorperazine |
10 mg (oral)
3 mg (buccal) |
30 – 40 mg (oral)
12 mg (buccal) |
| Domperidone |
10 mg |
40 mg |
* N.B. Paracetamol (500 mg) + caffeine (250 mg) may also be effective for some people (available over the counter).18, 25
Prescribe a triptan if simple analgesics were previously ineffective or migraine is severe
A triptan (5HT1-receptor agonist), i.e. rizatriptan or sumatriptan, is usually the next step for patients with migraine who have previously experienced an inadequate response to simple analgesics.2, 9, 28 A triptan can be prescribed first-line for patients experiencing more severe migraine.2, 9, 28 Triptans are most effective when taken as soon as possible after headache onset when the pain is still mild; they are unlikely to be effective if taken earlier during the aura phase.2, 9, 28 Triptans have demonstrated superior efficacy to simple analgesics, e.g. ibuprofen and naproxen, but are associated with a higher risk of medicine overuse headache, therefore, use should be limited to fewer than ten days per month.29, 31
Triptans are not suitable for all patients; they are contraindicated in people with hemiplegic migraine or migraine with brainstem aura, ischaemic heart disease, uncontrolled or severe hypertension and a range of other conditions (see NZF).30 They can also be associated with clinically significant medicine interactions, e.g. serotonin syndrome with concurrent use of medicines with serotonergic activity (rare), increased plasma concentration of rizatriptan with concurrent use of propranolol.30 See NZF for a full list of contraindications, cautions and medicine interactions, prior to prescribing rizatriptan or sumatriptan.
Triptans are generally well tolerated, but patients should be advised about potential adverse effects such as a tingling, heat or tightness sensation on the head, neck, chest or limbs.29, 30
Choosing between rizatriptan and sumatriptan
Rizatriptan and sumatriptan are considered equivalent options for the treatment of patients with acute migraine (see Table 1 for dosing).29 In practice, choice is predominantly based on formulation. Pharmaceutical dispensing data indicate that rizatriptan is most commonly prescribed in New Zealand, likely because the orodispersible tablet may improve absorption and provide a faster onset of action than traditional tablets.32 Anecdotally, patients tend to find rizatriptan more effective. Rizatriptan does not need to be taken with fluid; the tablet is placed on the tongue with dry hands and left to dissolve with saliva, then swallowed.30
Subcutaneous sumatriptan is usually reserved for patients with vomiting or severe migraine as it has a faster onset of action than tablets, however, it is associated with more adverse effects.2, 9 It can also be an option for patients who do not respond to oral triptans.9
Response to triptans varies. A second dose can be taken after two hours if pain was adequately treated, but migraine recurs;28, 29 patients who did not respond to the first dose should not take a second for the same episode.30 If a patient experiences an inadequate response to a triptan, review possible reasons for this, e.g. timing and route of administration.28 If the same triptan has been used without effect in two episodes, trial a different triptan next time.28, 29 Approximately 30% of people will not respond to any triptan.2
Combination treatment with a NSAID and triptan may be required
Combination treatment with a NSAID and a triptan is an option for patients with acute migraine, often for those who experience partial response to monotherapy with either medicine.2, 9, 28 Naproxen with sumatriptan is the most well studied combination, and has demonstrated superior efficacy to monotherapy.9, 31 However, combination treatment is associated with a high risk of medicine overuse headache, and therefore use should be limited to two days per week and fewer than eight days per month.28
Consider prescribing an antiemetic
An antiemetic should be considered for the treatment of patients with migraine-related nausea/vomiting (see Table 1 for dosing).2, 9, 11 Antiemetics can also improve gastric motility and enhance absorption of other medicines, therefore could be considered alongside other acute migraine treatments for patients without nausea/vomiting to reduce pain.2, 9, 11
A dopamine receptor antagonist should be used (e.g. metoclopramide, prochlorperazine, domperidone); metoclopramide and prochlorperazine have the greatest efficacy in acute migraine compared to other antiemetics.29 Also consider route of administration, e.g. buccal tablet of prochlorperazine (partly funded) or an injectable antiemetic such as metoclopramide, may be required for patients with vomiting.11 Ondansetron is not usually a first-line antiemetic for patients with migraine (unapproved indication) in the community as it does not have an effect on dopamine receptors;29 however, the orodispersible formulation may be helpful for patients if other antiemetics are ineffective or not tolerated.
Antiemetics are generally safe and well tolerated, but they can be associated with extrapyramidal effects, e.g. dystonia, and QT-interval prolongation, and so need to be used with caution in some patients.29, 30
A focus on menstrual migraine
Menstrual-related migraine is defined as migraine that occur between two days before and three days after menstruation, on at least two out of three consecutive menstrual cycles.2, 11 Menstrual migraine is believed to be related to a decrease in oestrogen, and is reportedly more severe and difficult to treat than migraine in general.16, 24, 28
An option for patients to reduce the frequency of menstrual migraine is to suppress ovulation, such as with continuous use of a combined oral contraceptive (unless aura is experienced) or progestogen-only pill (i.e. desogestrel).2, 16, 33
Combined oral contraceptives should not be used in patients who experience migraine with aura, as both factors increase stroke risk and in combination, the risk is considered to outweigh the benefit of treatment.2, 16, 34
Another option for patients who experience menstrual migraine is to stabilise fluctuating oestrogen levels, for example by prescribing transdermal oestrogen (with progesterone).28, 33, 34 N.B. Transdermal oestrogen avoids first-pass metabolism and generally does not increase stroke risk.33
Some patients may experience worsening migraine episodes while taking hormone treatments, particularly with high dose oestrogen; stop treatment if this occurs.24, 33
A triptan may also be considered as a short-term preventative if taken two days prior to menstruation until three days after bleeding begins (unapproved indication).2, 11 A long-acting triptan, e.g. frovatriptan, is recommended in international guidelines, however, these are not available in New Zealand. In practice, the transient effects of rizatriptan and sumatriptan may provide limited benefit in preventing menstrual migraine, but patients should not be discouraged from taking a triptan for this purpose if they find them to be effective.
For further information on selecting an oral contraceptive pill or hormone replacement treatment, see: https://bpac.org.nz/2021/contraception/oral-contraceptives.aspx and https://bpac.org.nz/2019/mht.aspx
Migraine during pregnancy and breast-feeding
During pregnancy, people tend to experience an improvement or remission in migraine.2, 9, 28 If migraine does occur, ideally manage with non-pharmacological approaches, however, if acute treatment is needed, paracetamol and metoclopramide are usually the safest options.9, 11, 28 Triptans may be considered in some cases, but it is best practice to discuss the patient with an obstetrician prior to prescribing.9, 28
Migraine prophylaxis is not usually recommended to be taken during pregnancy or breast-feeding due to potential risks to the fetus;20, 30, 35 seek obstetric advice for patients who experience frequent and severe migraine.11
For patients taking migraine prophylaxis who are planning pregnancy, consider the benefits and risks associated with the medicine. In most cases, migraine prophylaxis is likely to be appropriate to continue while trying to conceive (apart from topiramate and sodium valproate as these medicines are not suitable for females of childbearing potential). The medicine will likely need to be stopped once their pregnancy has been confirmed; seek specialist advice where needed.
Some people with migraine continue to experience frequent and severe episodes, despite optimal use of acute treatments, and therefore, require migraine prophylaxis.
Migraine prophylaxis is indicated for patients:2, 16, 35
- If they experience four or more migraine episodes or eight or more headache days per month
- Clinical judgement also applies, e.g. a patient with fewer but severe episodes may benefit from prophylaxis, whereas a patient with more frequent but mild episodes with limited impact on daily function may not require prophylaxis9
- If acute treatments are ineffective, not tolerated or contraindicated, or frequently used (and therefore they are at risk of medicine overuse headache)
Migraine prophylaxis is reportedly under-prescribed; a small New Zealand survey conducted in 2022 found that among those in whom migraine prophylaxis was indicated, fewer than 60% were taking it.36
Lifestyle changes and non-pharmacological interventions should be continued alongside migraine prophylaxis treatment, as well as medicines for acute migraine as needed.16, 20
Selecting a migraine preventative medicine
Conventional medicines for migraine prophylaxis include beta blockers (e.g. propranolol), antidepressants (e.g. amitriptyline), candesartan, topiramate and sodium valproate (Table 2).2, 9, 35 Newer medicines with high efficacy and tolerability are also available, e.g. CGRP-targeted treatments, but these are not funded (see: “Non-funded options for migraine prophylaxis are also available”).
The choice of migraine preventative medicine is an individualised decision, considering patient factors such as co-morbidities, risk factors, medicine interactions, prior treatment history, cost and patient preference (Table 2). There is no single approach to migraine prevention that is effective for every patient; a trial and error process is likely to be required.1 In general, to guide choice consider how the medicine may benefit the patient in other ways, e.g. prescribe a tricyclic antidepressant in a patient with concurrent fibromyalgia or an antihypertensive if they have raised blood pressure. Consider how the medicine will be tolerated, e.g. beta blockers or candesartan may cause light-headedness if prescribed in a young person with low blood pressure.
What to expect with migraine prophylaxis
Medicines for migraine prophylaxis should be initiated at a low dose and slowly up-titrated to the maximum tolerated dose (Table 2).2, 9 Advise patients that improvement may be gradual; response is unlikely to be rapid and it can take weeks for symptoms to improve.15, 20 Medicines should be trialled for at least two to three months (three to six months for CGRP-targeted treatments) at the maximum tolerated dose before assessing treatment response (see: “Assess treatment response and review ongoing need for prophylaxis”).2, 9, 15 Ask patients to continue completing a headache diary, as this will help to assess treatment response.2, 9
Table 2. Funded medicines commonly used for migraine prophylaxis.2, 9, 29, 35, 38
| Medicine |
Dosing |
Considerations (N.B. Check NZF for a full list of contraindications, cautions and adverse effects prior to prescribing.) |
| Cardiovascular |
Propranolol |
Initially, 40 mg, once or twice daily.30 Up-titrate as needed by the same amount per week to 80 – 160 mg, daily, in divided doses.30 |
- Propranolol is recommended as a first-line medicine for migraine prophylaxis in some guidelines.9 Propranolol can increase the plasma concentration of rizatriptan, therefore, rizatriptan should no longer be used for acute migraine treatment; sumatriptan or a NSAID may be prescribed instead.30
- Propranolol or metoprolol may be preferred for patients with co-morbid hypertension, arrhythmias or angina.30, 35 Propranolol may also be useful for patients with co-morbid anxiety.30, 35
- Propranolol and metoprolol are not usually suitable for patients with asthma, uncontrolled heart failure, hypotension or marked bradycardia.30 Some specialists advise caution with the use of beta blockers in patients with hemiplegic migraine due to historical case reports suggesting increased stroke risk. However, this relationship has not been fully established and is not included as a caution in the medicine data sheets.
- Propranolol and metoprolol can cause postural symptoms, drowsiness and bradycardia1, 30
N.B. Nadolol is also indicated for migraine prophylaxis; however, propranolol and metoprolol are more widely recommended likely in part due to stronger evidence of efficacy. See NZF for nadolol dosing information and other considerations. |
Metoprolol succinate |
Initially, 47.5 mg, once daily.30 Up-titrate as needed to 95 – 190 mg, daily.30
See NZF for dosing information on metoprolol tartrate. |
Candesartan
(unapproved indication) |
Dosing depends on baseline blood pressure. Initially 4 – 6 mg, once daily.24 Up-titrate as needed by 4 mg per week to 16 mg (up to 32 mg if concurrent hypertension), once daily.24, 35 |
- May be preferred for patients with co-morbid hypertension or heart failure29, 35
- Can cause hypotension and dizziness30, 35
|
| Antidepressants |
Amitriptyline
(unapproved indication) |
Initially, 10 mg, once daily at night.30 Up-titrate as needed to 50 – 75 mg, once daily (maximum 150 mg, daily).30 |
- Amitriptyline may be preferred for patients with co-morbid depression, neuropathic pain or sleep disturbances10, 29, 35
- In practice, venlafaxine should only be considered for migraine prophylaxis in patients with a co-morbid mood disorder. If migraine is not adequately controlled with venlafaxine but the patient’s mood is, continue the medicine for the purpose of mood management and consider trialling an alternative for migraine prophylaxis.
- Amitriptyline and venlafaxine are not suitable for patients with arrhythmias or conditions associated with a high risk of cardiac arrhythmias.30 Venlafaxine is also not suitable for patients with uncontrolled hypertension.30
- Adverse effects of amitriptyline may limit use, e.g. weight gain, constipation, drowsiness.1, 15, 30 Venlafaxine may be better tolerated (if the patient has a co-morbid mood disorder), or a less sedating tricyclic antidepressant, e.g. nortriptyline (unapproved indication).9, 16, 29
|
Venlafaxine
(unapproved indication) |
Dose according to the co-morbid mood disorder. Up-titrate the dose until the mood disorder is adequately controlled. See NZF for specific dosing information. |
| Anti-seizure |
Topiramate |
Initially, 25 mg, once daily at night for one week.30 Up-titrate as needed in 25 mg increments per week to 50 – 100 mg, daily, in two divided doses (maximum 200 mg, daily).30 |
- Sodium valproate and topiramate are not suitable for females of childbearing potential unless a highly effective contraceptive method is used, e.g. intrauterine device.30 Males should also use effective contraception when taking sodium valproate.30
- Use topiramate and sodium valproate with caution in patients with a history of psychiatric disorders: monitor for changes in mood, including depression and suicidal ideation30
- Topiramate can cause weight loss, paraesthesia, cognitive impairment and nephrolithiasis1, 30, 35
- Sodium valproate can cause weight gain, drowsiness, tremor, hair loss and abnormal laboratory findings, e.g. abnormal liver function tests1, 30, 35
|
Sodium valproate
(unapproved indication) |
Initially, 200 mg, twice daily.30 Up-titrate as needed to 1.2 – 1.5 g, daily, in divided doses.30 |
N.B. Clonidine and pizotifen are also indicated for migraine prophylaxis, however, they are no longer routinely prescribed for this purpose in New Zealand as clonidine can aggravate depression and cause insomnia, and there is limited evidence supporting benefit with pizotifen compared to other options.30, 35
Non-funded options for migraine prophylaxis are also available
Newer medicines have been developed specifically for migraine prophylaxis that target the neuropeptide CGRP, which is commonly implicated in migraine pathophysiology.39, 40 There are two classes of CGRP-targeted medicines:30
CGRP monoclonal antibodies (subcutaneous injection). Erenumab (Aimovig), galcanezumab (Emgality) and fremanezumab (Ajovy) are approved in New Zealand for the prophylaxis of migraine in adults. Erenumab binds to the CGRP receptor, whereas galcanezumab and fremanezumab bind to the CGRP ligand. These medicines should generally be initiated by a neurologist or other clinician with experience in the management of migraine.30 However, in-person access to a neurologist is limited. Primary care clinicians can initiate these medicines if they feel confident, or seek advice from a neurologist prior to prescribing. Erenumab and galcanezumab are administered monthly; fremanezumab can be dosed monthly or quarterly.
Small-molecule CGRP receptor antagonists, known as gepants. Atogepant (Aquipta) is the only gepant available in New Zealand. It is an oral tablet taken once daily, indicated for the prophylaxis of migraine in patients with at least four migraine days per month.
None of these medicines are currently funded in New Zealand. However, the option of self-funding treatment should still be discussed so patients can consider it depending on their individual circumstances. The monthly cost of galcanezumab, fremanezumab and atogepant is similar (in the range of $300 – $350); erenumub costs more per month (over $600). Galcanezumab will have a higher initial cost as a loading dose is required. Information on the approximate costs of CGRP-targeted treatments is available from the Migraine Foundation. Cost will also vary between pharmacies; patients may wish to check costs with several pharmacies prior to having their prescription dispensed.
CGRP-targeted treatments are effective and may be better tolerated
CGRP-targeted treatments are reported to be the most effective medicines for migraine prophylaxis, e.g. a randomised controlled trial demonstrated a greater reduction in monthly migraine days with erenumab (–5.86) compared to topiramate (–4.02), and more participants experienced a ≥ 50% reduction in monthly migraine days (55% versus 31%).37, 41 The strong evidence of efficacy has led to their recommendation as first-line options for migraine prevention by the European Headache Federation and the American Headache Society.39, 42
CGRP-targeted treatments are also often better tolerated than conventional migraine preventatives; if adverse effects are experienced, they are usually mild in nature, e.g. constipation, fatigue, nausea, injection site reactions (with CGRP monoclonal antibodies).37, 40 Worsening of pre-existing hypertension and recurrence or worsening of Raynaud’s phenomenon has been reported with CGRP-targeted treatments, therefore, they should be used with caution in patients with these conditions. Erenumab should also be used with caution in patients with a history of constipation, or concurrent use of medicines that cause constipation.
Selecting a CGRP-targeted treatment
All CGRP-targeted medicines are considered to be similarly effective, including injectable and oral formulations.43, 44 As with conventional migraine prophylactic medicines, finding a CGRP-targeted treatment that is most effective for the patient is a trial and error process. These treatments should be taken for three to six months before assessing response.20 Initial selection of a medicine can be based on the patient’s preference regarding route of administration, dosing frequency and cost. However, how effective a medicine is will determine its value for money, so cost comparison alone should not be a deciding factor.
For many patients, CGRP-targeted treatments will not be affordable and conversations about their superior effectiveness will be distressing. Therefore, clinicians must balance the need for patients to be provided with information about all available options, with optimism about managing migraine with funded treatments.
Botulinum toxin type A: An option for patients with chronic migraine
Botulinum toxin type A or onabotulinumtoxinA (BOTOX) purified neurotoxin complex is indicated for the prophylaxis of headache in adults with chronic migraine.30 Evidence has demonstrated that it may reduce the number of migraine days per month compared to placebo.29, 45 The mechanism of action for reducing migraine frequency is not fully understood, but the inhibition of neurotransmitters/neuropeptides involved in migraine pathogenesis is believed to be involved to some extent.15, 29
Botulinum toxin type A treatment is generally accessed via private clinics; therefore cost will be a barrier for many patients. Advise patients to select a clinic that uses the PREEMPT protocol for administration as this is specific to chronic migraine, and differs from cosmetic use of botulinum toxin: it involves over 30 injections around the forehead, head and neck, every 12 weeks.2, 29 It can take two to three sessions for patients to notice an effect.
In some cases, botulinum toxin type A treatment may be given in a neurology outpatient setting (funded; availability varies between hospitals in New Zealand); however, this is only for very select patients with severe chronic migraine.
Assess treatment response and review ongoing need for prophylaxis
Patients starting a preventative migraine medicine should be followed up regularly while the dose is up-titrated; reviews can then reduce in frequency over time.8, 20 At each review, assess adherence, adverse effects, change in frequency and severity of migraine episodes and impact on quality of life, as well as reinforce lifestyle measures.9, 20 Reviewing the patient’s headache diary can help with evaluating treatment progress, as well as repeating questionnaires that were completed at diagnosis, e.g. MIDAS.2, 9, 35
A 30 – 50% reduction in severity and frequency of headache is generally considered an adequate response to treatment.8–10 However, patients who do not achieve this metric but do experience other benefits, e.g. improved quality of life, functional ability, may still be considered as having an adequate response to the medicine, particularly if it is well tolerated.15, 35
Next steps for patients with an inadequate response
After three months of treatment (or six months with CGRP-targeted treatments) if there is an inadequate response at the maximum tolerated dose, consider switching to an alternative medicine or trialling combination treatment with an additional migraine preventative.15, 20, 45 There is no specific guidance available on which medicine combinations are the most effective; consider patient co-morbidities, medicines mechanism of action and interactions when deciding on which combination(s) to trial. Discussion with, or referral to, a neurologist is usually appropriate for patients who experience an inadequate response to multiple migraine preventative medicines.9 Patients will require ongoing support and encouragement in persisting with finding a migraine preventative medicine that works for them.
Determine whether ongoing prophylaxis is indicated
Migraine prophylaxis will not be required long-term for all patients. Withdrawal can be useful to determine whether the patient’s migraine frequency has reduced on its own and whether prophylactic treatment is still indicated, e.g. patients may have made positive lifestyle changes that mean they now experience fewer migraine episodes.
Guidelines advise that patients who have responded well to migraine prophylaxis should continue with treatment for a further 6 – 12 months before attempting a gradual withdrawal.2, 9, 11 This period helps patients to re-gain confidence and engage with previously lost activities, e.g. exercise, socialisation, employment. During this time, ask patients to reflect on what has been working well and if any triggers can be identified if they did experience an occasional migraine. This is an opportunity for the patient to build understanding and knowledge of their condition and improve their emotional health, e.g. developing resilience.
In practice, many patients will fear discontinuing migraine prophylaxis; use clinical judgement and consider the patient’s goals of treatment and preferences when determining the optimal time to trial withdrawal. In some cases, remaining on migraine prophylaxis for longer than 12 months may be appropriate. Withdrawing treatment in a step-wise manner can help patients gain further confidence in stopping migraine prophylaxis. Advise patients of the possibility that migraine frequency may worsen as the medicine is withdrawn (particularly with CGRP-targeted treatments); explain that the dose may need to be temporarily increased back to the previous one during the tapering process, or the medicine re-started again (if the threshold for preventative treatment is met, see: “The prophylaxis of migraine”).35 Ensure acute treatments are available to bridge any episodes.
We invited co-founder of the Migraine Foundation New Zealand, Dr Fiona Imlach, to share her personal story to help healthcare professionals understand the impacts of migraine. Some passages have been edited.
Migraine is a lifelong journey, and everyone’s experience is different
I’ve had episodic migraine for most of my life. It changed from an attack once every few months or so to an average of three or more times a week in my mid-20s. This continued pretty much unabated into my 40s.
Migraine restricted my career ambitions – I had to choose jobs that allowed some degree of working flexibility and I limited the amount of time I worked. So many days I gritted through a migraine at the office, depleting all my reserves so that when I got home, I was a useless wreck, barely able to crawl into bed, let alone have a coherent conversation with my partner. I let hobbies and creative pursuits slip away, because I only had enough energy to attend to the basics – exercise, healthy eating, sleeping, trying to keep connections with family and friends. The silver lining was being forced to prioritise my physical and mental health. If I don’t exercise or get enough sleep, or if I am overwrought by some drama, the ramifications are usually prompt.
I sometimes think of migraine as my health watchdog, that bites me when I stray too far from the path of well-being and zen. But often the dog goes rabid, and bites me when there is no need.
What works for me might not work for you
Lack of sleep, emotional stress, alcohol and over-exertion are my biggest migraine triggers. But not always and not inevitably. I think of triggers as pushing me over a threshold into a migraine attack – but some days, the threshold is high and it takes more than one adverse factor to reach it.
My go-to pain relievers are NSAIDs and/or a triptan. I might also take coffee, ginger tablets (or ginger beer or tea) and an anti-nausea tablet. Most of the time, this works. I put myself to bed early, if I can. Sometimes, the only solution is as much sleep as I can manage to get when it feels like a couple of knives are stuck in my skull.
There is no easy fix
I’ve tried almost every migraine preventative medicine available. None of them made a significant or long-lasting difference and most had unpleasant adverse effects. Supplements, Chinese and Ayurvedic medicines, Botox, acupuncture, occipital nerve injection, physiotherapy, alternative therapies, dietary restrictions: nothing worked. No matter what I did, I still had headache on around half the days in the month and other migraine symptoms on the rest of the month, particularly fatigue, nausea and brain fog.
Some things I’ve found helpful in reducing the severity of attacks or helping me recover more quickly include biofeedback (teaching me how to breathe in a way that calms my body down), yoga, exercise, a strict bed time so I get enough sleep (especially important for menopausal-related hot flushes and insomnia), and transcutaneous electrical nerve stimulation machine.
CGRP-targeted treatments were the first migraine preventative treatment that worked for me, with no adverse effects. I’ve gone from chronic migraine to now having five headache days in the last month, but only needing to take one triptan. Previously, I was always weighing up when to take a triptan, shadowed by the ever-present fear of medicine overuse headache. These new medicines have been life changing. They are not a cure, and they haven’t worked 100% but they have suppressed the migraine dragon in my brain.
My GP has been very supportive and willing to try new things, but I couldn’t avoid feeling that I was untreatable when the medicines didn’t work for me, and that this was somehow my fault, and entirely my problem when the medical establishment ran out of options. Having more GPs who take a special interest in migraine management and related pain issues could be helpful. It’s an unfortunate truth that pain loves company, and chronic migraine is not infrequently coupled with other diagnoses, such as fibromyalgia, irritable bowel syndrome, endometriosis, low back pain, bladder and pelvic pain. More research and understanding of the nature of pain and why migraine occurs is desperately needed. Fast-tracking the approval and funding of new migraine treatments would be a tremendous boon.
Keep trying and don’t lose hope
I’ve grown a little wiser over the years, and a little more forgiving of myself. I’ve lowered my expectations of what I can achieve, but with an attitude of permission and equanimity, not judgment and disappointment. I’ve cultivated gratitude for all the amazing things I have still been able to do, experience and share.
There is always hope and positive actions that can be taken. Even when migraine becomes chronic, the pain can wax and wane and you can still be proud of achieving the task of getting through the day. Goals may shrink, but your value as a person does not.
To read Fiona’s full story, see: migrainefoundation.org.nz/fiona-wellington/
For further information on the Migraine Foundation Aotearoa New Zealand, see: migrainefoundation.org.nz/






