
B-QuiCK: Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS)
Assessment and diagnosis
First, establish the nature, duration, frequency and severity of symptoms:
- Pelvic or genitourinary pain is reported in most cases, in one or multiple locations, e.g. the perineum, penis or testes (especially penile tip), groin, rectum, lower back or abdomen. Pain on or after urination or ejaculation or suprapubic pain may also occur. Patients may describe feeling like they are “sitting on a hot poker”.
- Lower urinary tract symptoms may include hesitancy, urgency, dysuria, haematospermia
- Psychological symptoms include co-morbid depression and anxiety
- Sexual dysfunction such as erectile dysfunction, premature or delayed ejaculation and decreased libido may be present
Relevant history includes co-morbidities such as diabetes or immunocompromise, previous pelvic injury, recent diagnosis of a UTI or STI, known BPH, recent urological procedures and sexual history.
The diagnosis of CP/CPPS is based on recognising a pattern of symptoms that are not explained by any other diagnoses:
- Consider CP/CPPS in a patient if pelvic or genitourinary pain has been present for at least three of the past six months and urine culture results are negative
- Differential diagnoses include chronic bacterial prostatitis, BPH, bladder, colorectal or prostate cancer, prostatic abscess, pelvic floor dysfunction
Symptom management
- CP/CPPS is a chronic condition that cannot be cured but the symptoms can be successfully managed
- Tailor treatment to the individual patient’s predominant symptoms with the overall goal of improving their quality of life
- Prescribe a combination of first-line options for four to six weeks; obvious symptom improvement may not be seen until the end of this period
- Antibiotic treatment is not recommended
- Beneficial medicines should be continued long-term
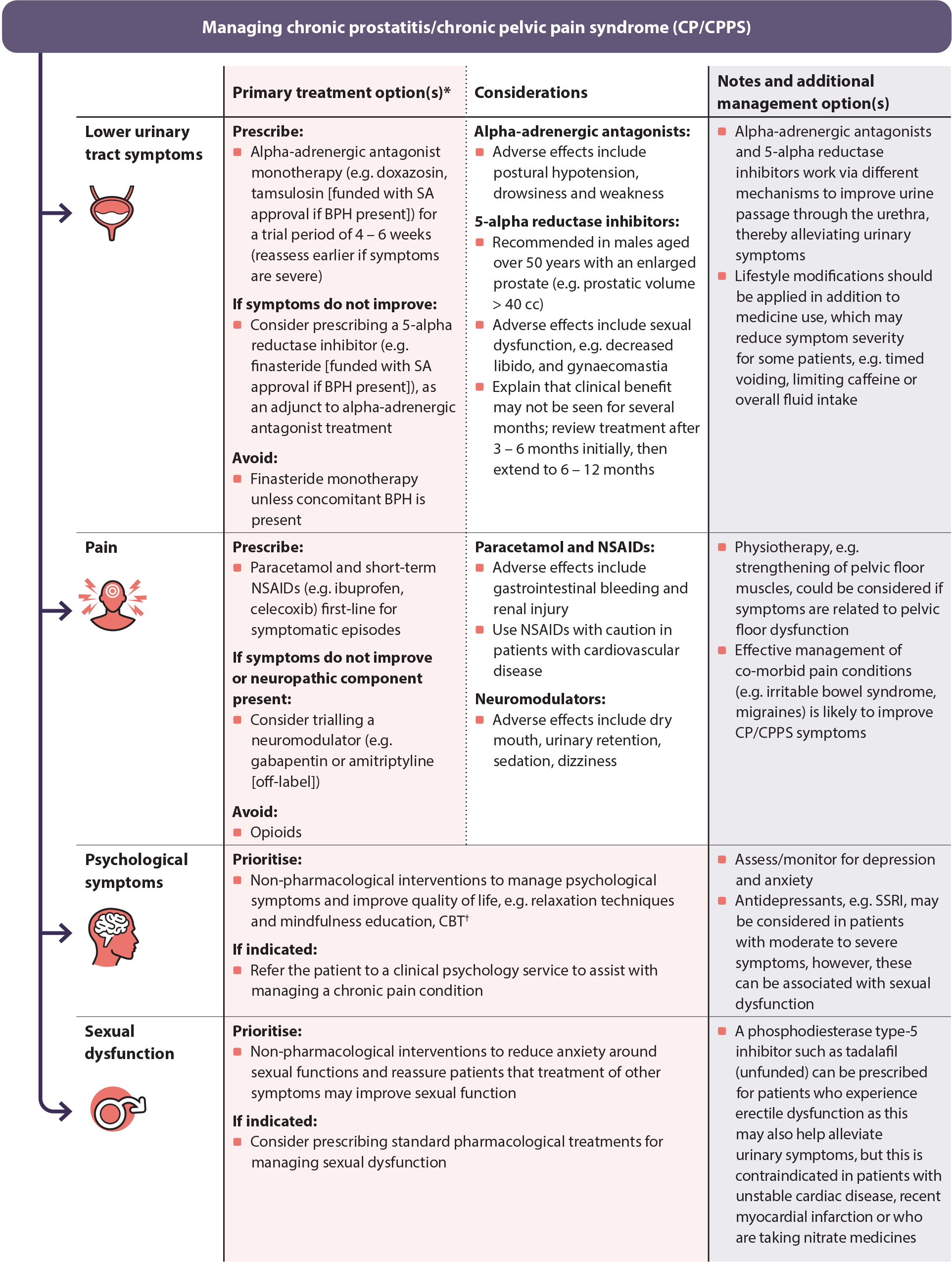
Figure 1. Symptom-based management of chronic prostatitis/chronic pelvic pain syndrome.6, 14, 20 ,24, 25
* For further information on specific dosing of medicines for CP/CPPS, see: https://nzf.org.nz/nzf_4259
† Free online (non-specific) CBT courses are available from: https://www.justathought.co.nz/ and https://beatingtheblues.co.nz/
BPH = benign prostatic hyperplasia; CBT = cognitive behavioural therapy; SA = Special Authority; SSRI = selective serotonin reuptake inhibitor
Follow up
Arrange follow-up four to six weeks after initial presentation to evaluate the patient’s response to treatment
- Assess how the patient is coping with the psychological impacts of their symptoms
Early referral is recommended for patients who do not report symptom improvement following initial treatment or if pelvic pain or lower urinary tract symptoms are causing a significant impact on their quality of life
- Consider trialling second-line interventions while awaiting non-acute urology assessment, e.g. a 5-alpha reductase inhibitor or amitriptyline





