Published: July, 2024 | Review date: July, 2027
This audit identifies younger male patients, who are less likely
to present to primary care, to assess whether they have been
offered a sexual health check within the past 12 months.
This audit also provides an opportunity to check the HPV
vaccination status of these patients and offer vaccination
where appropriate.
N.B. The term “male” is used to describe the biological sex of the
patient population who are the focus of this audit. However,
we acknowledge that this may not reflect the identity of
all patients, which will include transgender girls or women,
intersex and non-binary individuals.
Rates of sexually transmitted infections (STIs) are high in New
Zealand. Chlamydia is the most commonly reported bacterial
STI.1 Small increases in the number of infectious syphilis
and gonorrhoea cases have been reported recently; both of
which disproportionately affect men who have sex with men
(MSM).1 Genital warts are more common in males, but overall
diagnoses continue to decrease following inclusion of the
human papillomavirus (HPV) vaccination (Gardasil 9) in the
National Immunisation Schedule in 2008.1
The highest rates of STIs are typically reported in younger
adults and adolescents, due to an increased prevalence
of higher risk sexual behaviours, e.g. frequently changing
or concurrent sexual partners, condomless sex. As these
infections can be asymptomatic, increased testing is essential
to prevent complications developing and transmission of
infections to others by enabling prompt treatment. Annual
STI testing is recommended for all sexually active people aged
< 30 years; more frequent testing may be indicated for certain
groups, e.g. people who have multiple sexual partners, MSM.
STI testing rates are typically lower for males than females.
Younger males in particular may rarely attend primary
care, therefore, any consultation should be considered as a
potential opportunity to initiate a discussion about sexual
health and offer STI testing as appropriate. This is also an
opportunity to check HPV vaccination status and discuss
vaccination with those who are eligible* but have not been
immunised, e.g. those who missed out on the school-based
programme.
*HPV vaccination is recommended and funded for all people aged 9
– 26 years. The vaccine can be administered (not funded) to people
aged 27 years and over if they have not been vaccinated before and
are likely to benefit, e.g. MSM, those with HIV infection or people who
are newly sexually active.
References:
- The Institute of Environmental Science and Research Ltd (ESR).
Sexually transmitted infections in New Zealand: supplementary
annual surveillance report 2022. 2023. Available from: https://www.esr.cri.nz/digital-library/sexually-transmitted-infections-annual-surveillance-report-2022/ (Accessed Jul, 2024).
For further information on how to perform a sexual
health check, see: bpac.org.nz/BPJ/2013/April/how-to-guide-sexual-health.aspx
For latest recommendations on testing, see: sti.guidelines.org.nz/sexual-health-check/
For guidance on antibiotic management of chlamydia,
gonorrhoea, Mycoplasma genitalium and syphilis infections
in primary care, see: bpac.org.nz/antibiotics/guide.aspx
For further information on HPV vaccination, including
the vaccination schedule and groups eligible for funded
vaccination, see: bpac.org.nz/2019/hpv.aspx
Summary
This audit identifies male patients aged 16 – 30 years who
have presented to primary care in the past 12 months to
assess whether they have been offered a sexual health
check or had appropriate STI testing. They should also have
a record of a completed HPV vaccination course or an offer of
immunisation to those who are eligible but have not yet been
vaccinated or completed the course.
Recommended audit standards
Ideally, all male patients aged 16 – 30 years should have
documented evidence in their patient record of having
been offered a sexual health check or had appropriate STI
testing in the previous 12 months. Any patients who do
not have the recommended information in their clinical
notes should be flagged for review. They should also have
a record of a completed HPV vaccination course or an offer
of vaccination (at any time). Any patients who do not have
the recommended information in their clinical notes and are
eligible for vaccination (i.e. aged 26 years and under) should
be flagged for review, e.g. a discussion about vaccination
at their next appointment. Also consider offering HPV
vaccination to patients aged 27 years and over if they have
not been vaccinated before and are likely to benefit (however,
this would not be funded).
 Alternatively, consider a “working audit” where the data sheet is filled in over time opportunistically during consultations for
any reason with an eligible patient until the required number
of patients has been reached. If conducting a “working audit”
and there is no record of a recent sexual health check or a
discussion regarding HPV vaccination in the patient’s clinical
notes, this should be undertaken at the time, or a future
appointment booked.
Alternatively, consider a “working audit” where the data sheet is filled in over time opportunistically during consultations for
any reason with an eligible patient until the required number
of patients has been reached. If conducting a “working audit”
and there is no record of a recent sexual health check or a
discussion regarding HPV vaccination in the patient’s clinical
notes, this should be undertaken at the time, or a future
appointment booked.
Eligible patients
All male patients within the practice who are aged 16 – 30
years and have attended primary care for any reason in the
past 12 months are eligible for this audit.
Identifying patients
For the conventional audit, you will need to have a system in
place that allows you to identify eligible patients and audit
their clinical notes. Many practices will be able to do this by
running a ‘query’ through their PMS to find all male patients
aged 16 – 30 years. The notes of identified patients will need
to be reviewed and those who have attended a primary care
consultation within the past 12 months selected for the audit.
If conducting a “working audit” fill in the data sheet when you
have a consultation for any reason with an eligible patient
until the required number of patients has been reached.
N.B. To increase vaccination uptake in this key population, consider
running a separate PMS ‘query’ to identify all male patients aged 16 – 30
years enrolled in the practice who have not yet received HPV vaccination
(or completed the course) and flag for discussion at the next appointment.
Sample size
The number of eligible patients will vary according to your
practice demographic. A sample size of 30 patients is sufficient
for this audit; a smaller sample size may be necessary if
conducting a working audit.
N.B. The timeframe of the audit can be extended beyond 12 months if an
insufficient number of patients are initially identified.
Criteria for a positive outcome
For a positive result for the audit, the patient’s clinical notes
should contain the following:
- Record of a discussion offering a sexual health check or
a record of recommended STI testing for their clinical
circumstances in the past 12 months; AND
- Record of completed HPV vaccination course or an offer
of vaccination at any time
Data analysis
Use the sheet provided to record your data.
In the conventional audit (Data sheet A), a positive result is
any patient who has documented evidence in their notes of
an offer of a sexual health check or a record of appropriate STI
testing in the past 12 months and a record of HPV vaccination
or a discussion offering vaccination to those in whom it is
recommended, at any time. The percentage achievement
can be calculated by dividing the number of patients with a
positive result by the total number of patients audited.
In the working audit (Data sheet B), aim to carry out a sexual
health check for as many eligible patients as possible. HPV
vaccination should also be offered to all patients in whom
vaccination is recommended but they have not yet received
it or completed the course.
Clinical audits can be an important tool to identify where gaps exist between expected and actual performance. Once completed, they can provide ideas on how to change practice and improve patient outcomes. General practitioners are encouraged to discuss the suitability and relevance of their proposed audit with their practice or peer group prior to commencement to ensure the relevance of the audit. Outcomes of the audit should also be discussed with the practice or peer group; this may be recorded as a learning activity reflection if suitable.
The Plan, Do, Study, Act (PDSA) model is recommended by the Royal New Zealand College of General Practitioners (RNZCGP) as a framework for assessing whether a clinical audit is relevant to your practice. This model has been widely used in healthcare settings since 2000. It consists of two parts, the framework and the PDSA cycle itself, as shown in Figure 1.
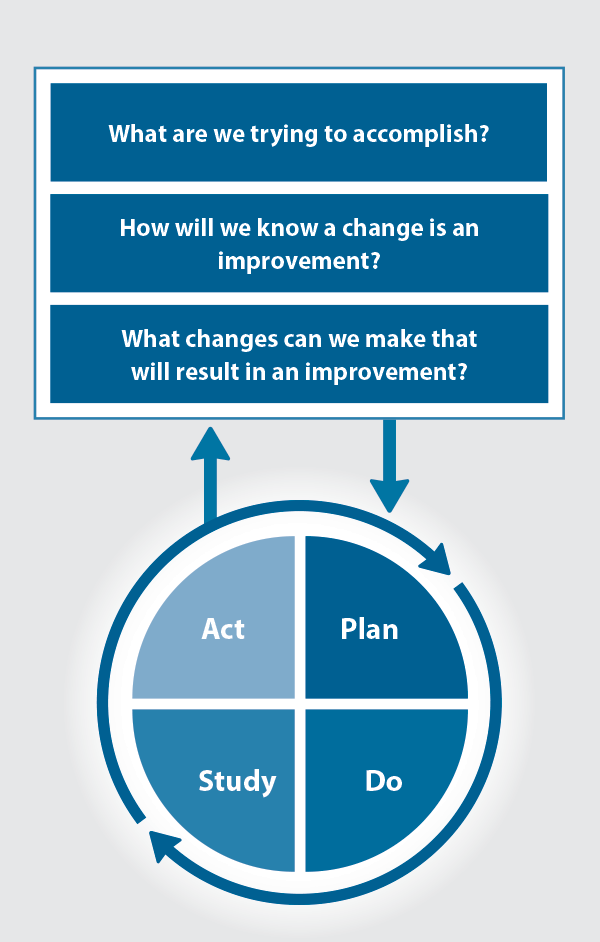
Figure 1. The PDSA model for improvement.
Source: Plan, Do, Study, Act (PDSA) cycles and the model for improvement
1. The framework
This consists of three questions that help define the “what” and “how” of an improvement project (in this case an audit).
The questions are:
- "What are we trying to accomplish?" – the aim
- "How will we know that a change is an improvement?" – what measures of success will be used?
- "What changes can we make that will result in improvement?" – the concept to be tested
2. The PDSA cycle
This is often referred to as the “engine” for creating, testing and carrying out the proposed changes. More than one cycle is usually required; each one is intended to be short, rapid and frequent, with the results used to inform and refine the next. This allows an ongoing process of continuous learning and improvement.
Each PDSA cycle includes four stages:
- Plan – decide what the change to be tested is and how this will be done
- Do – carry out the plan and collect the data
- Study – analyse the data, assess the impact of the change and reflect on what was learned
- Act – plan the next cycle or implement the changes from your plan

Claiming credits for Te Whanake CPD programme requirements
Practice or clinical audits are useful tools for improving clinical practice and credits can be claimed towards the Patient Outcomes (Improving Patient Care and Health Outcomes) learning category of the Te Whanake CPD programme, on a two credit per learning hour basis. A minimum of 12 credits is required in the Patient Outcomes category over a triennium (three years).
Any data driven activity that assesses the outcomes and quality of general practice work can be used to gain credits in the Patient Outcomes learning category. Under the refreshed Te Whanake CPD programme, audits are not compulsory and the RNZCGP also no longer requires that clinical audits are approved prior to use. The college recommends the PDSA format for developing and checking the relevance of a clinical audit.
To claim points go to the RNZCGP website: www.rnzcgp.org.nz
If a clinical audit is completed as part of Te Whanake requirements, the RNZCGP continues to encourage that evidence of participation in the audit be attached to your recorded activity. Evidence can include:
- A summary of the data collected
- An Audit of Medical Practice (CQI) Activity summary sheet (Appendix 1 in this audit or available on the
RNZCGP website).
N.B. Audits can also be completed by other health professionals working in primary care (particularly prescribers), if relevant. Check with your accrediting authority as to documentation requirements.





