Published: May, 2026 | Review date: May, 2029
This audit helps primary healthcare professionals ensure patients diagnosed with CKD are prescribed optimal treatment.
A combination of medicines, termed the “four pillars” approach, is increasingly being recognised as the new standard of care for managing patients with CKD, similar to what is now considered standard practice for heart failure.
The “four pillars” of CKD treatment are:
- An ACE inhibitor/ARB; and
- A SGLT-2 inhibitor; and/or
- A GLP-1 receptor agonist; and/or
- A non-steroidal MRA (not routinely available in New Zealand)
The benefits of combination treatment have primarily been demonstrated in people with CKD and diabetes, however, evidence in those without diabetes is increasing, particularly for SGLT-2 inhibitors. More studies are needed to determine the role of GLP-1 receptor agonists in CKD management for people without diabetes; emerging evidence suggests benefit with semaglutide in those who are overweight/obese. The absolute benefits of combination treatment with all four medicines in patients with CKD are greatest in those at high risk of progression, e.g. with significantly reduced eGFR or albuminuria. Further research is required to determine the optimal timing and intensity of the “four pillars” treatment across all patient groups with CKD, e.g. those at lower risk of progression. However, international evidence suggests that the “four pillars” are underutilised among people with CKD who need them the most.
In New Zealand, medicines availability and Special Authority funding restrictions influence the ability to adopt the “four pillars” approach. SGLT-2 inhibitors are only funded for some patients with type 2 diabetes or heart failure and GLP-1 receptor agonists for some patients with type 2 diabetes (and not together, unless empagliflozin is prescribed for heart failure), and non-steroidal MRAs are not routinely available outside of a clinical trial setting. The option of self-funding treatment with a SGLT-2 inhibitor or GLP-1 receptor agonist should still be discussed, so that patients can consider it depending on their individual circumstances.
Prescribing decisions can be made using a risk-based approach, prioritising the addition of key medicines to the patient’s regimen where possible; the definition of optimal treatment will therefore differ between patients with CKD (see box).
Defining optimal treatment for CKD
Optimal treatment for CKD differs between patients depending on factors such as eGFR, underlying cause of CKD (e.g. type 2 diabetes), other co-morbidities (e.g. heart failure) and individual preferences (e.g. financial circumstances). The following table can be used as a guide to help determine whether the treatment regimen for a patient with CKD is optimal.
| |
Yes |
No |
Other |
|
Patient prescribed maximum tolerated dose of an ACE inhibitor or ARB
|
|
|
- Contraindicated
- Not tolerated
|
|
Patient prescribed empagliflozin
|
|
|
- Contraindicated
- Not tolerated
- Not suitable for another clinical reason, e.g. eGFR < 20 mL/min/1.73 m2
- Special Authority criteria not met and self-funding not possible
|
|
Patient prescribed GLP-1 receptor agonist
|
|
|
- Contraindicated
- Not tolerated
- Not suitable for another clinical reason, e.g. does not have type 2 diabetes, eGFR < 15 mL/min/1.73 m2
- Special Authority criteria not met and self-funding not possible
|
|
Optimal treatment is zero ticks in “No” column
|
Opportunistically re-visit empagliflozin and GLP-1 receptor agonist funding. For patients in whom empagliflozin or dulaglutide/liraglutide is not currently funded and the option of self-funding treatment has been discussed, but is not possible, add a note to their clinical record to periodically re-check if they now meet criteria for funded treatment, or re-visit the conversation of self-funding.
Summary
This audit identifies patients with CKD to determine if they are currently prescribed optimal treatment. Optimal treatment for CKD varies between patients (see box). The topic of this audit and the potential difficulties in accurately searching for and identifying patients with CKD (and those not coded appropriately), as well as finding necessary information about relevant medicines including funding discussions, makes a working (opportunistic) audit the best choice.
When an eligible patient presents for any reason during the allocated time frame for the audit, check if their current treatment regimen for CKD is optimal. Ideally, this is determined during consultation with the patient as this will avoid having to review their clinical notes later (the audit data sheet can be competed after the consultation). If their treatment is optimal, no further action is required. If their treatment regimen could be optimised, either discuss this at the time, book a future appointment or add a note to their clinical record to discuss when they next present.
Recommended audit standards
Most patients with CKD should be established on an ACE inhibitor or ARB, empagliflozin and/or dulaglutide or liraglutide unless:
- There are contraindications or clinical justification for why one or more of the medicines is not appropriate, e.g. eGFR < 20 mL/min/1.73 m2, not tolerated, patient does not have type 2 diabetes (dulaglutide/liraglutide not indicated)
- They do not meet criteria for Special Authority approval, and self-funding has been discussed and is not possible
Eligible patients
All patients with CKD are eligible for this audit.
Identifying patients
 This is a working audit where you identify eligible patients opportunistically during a consultation for any reason over the course of an allocated time frame.
This is a working audit where you identify eligible patients opportunistically during a consultation for any reason over the course of an allocated time frame.
Sample size
The number of eligible patients will vary according to your practice demographic. A small sample size, e.g. 10 – 15 patients, may be necessary to complete the audit within your planned time frame. All eligible patients should be reviewed subsequently over time.
Criteria for a positive outcome
A positive result is achieved if an eligible patient is prescribed optimal treatment for CKD. If their treatment regimen for CKD could be optimised, either discuss this at the time or book a future appointment. For patients who do not want to book a follow-up appointment, add a note to their clinical record to re-visit optimising treatment when they next present for a consultation.
Data analysis
Use the sheet provided to record your data. The percentage achievement can be calculated by dividing the number of patients with a positive outcome by the total number of patients audited.

This publication was supported by an unrestricted educational grant by Boehringer Ingelheim. The publication was independently written and Boehringer Ingelheim had no control over the content. The views expressed in this publication are those of the author and not necessarily those of Boehringer Ingelheim.
Clinical audits can be an important tool to identify where gaps exist between expected and actual performance. Once completed, they can provide ideas on how to change practice and improve patient outcomes. General practitioners are encouraged to discuss the suitability and relevance of their proposed audit with their practice or peer group prior to commencement to ensure the relevance of the audit. Outcomes of the audit should also be discussed with the practice or peer group; this may be recorded as a learning activity reflection if suitable.
The Plan, Do, Study, Act (PDSA) model is recommended by the Royal New Zealand College of General Practitioners (RNZCGP) as a framework for assessing whether a clinical audit is relevant to your practice. This model has been widely used in healthcare settings since 2000. It consists of two parts, the framework and the PDSA cycle itself, as shown in Figure 1.
1. The framework
This consists of three questions that help define the “what” and “how” of an improvement project (in this case an audit).
The questions are:
- "What are we trying to accomplish?" – the aim
- "How will we know that a change is an improvement?" – what measures of success will be used?
- "What changes can we make that will result in improvement?" – the concept to be tested
2. The PDSA cycle
This is often referred to as the “engine” for creating, testing and carrying out the proposed changes. More than one cycle is usually required; each one is intended to be short, rapid and frequent, with the results used to inform and refine the next. This allows an ongoing process of continuous learning and improvement.
Each PDSA cycle includes four stages:
- Plan – decide what the change to be tested is and how this will be done
- Do – carry out the plan and collect the data
- Study – analyse the data, assess the impact of the change and reflect on what was learned
- Act – plan the next cycle or implement the changes from your plan
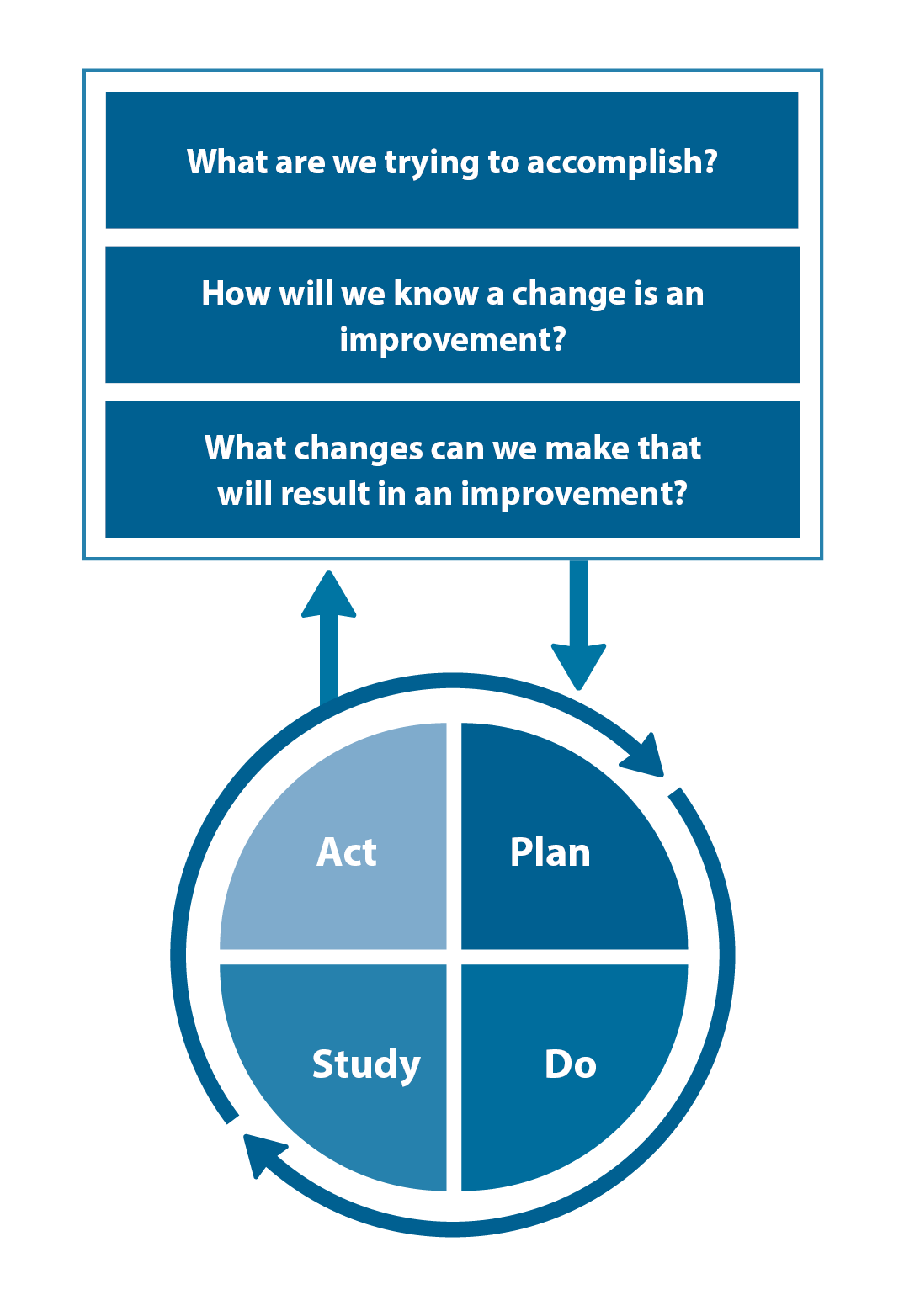
Figure 1. The PDSA model for improvement.
Source: Plan, Do, Study, Act (PDSA) cycles and the model for improvement

Claiming credits for Te Whanake CPD programme requirements
Practice or clinical audits are useful tools for improving clinical practice and credits can be claimed towards the Patient Outcomes (Improving Patient Care and Health Outcomes) learning category of the Te Whanake CPD programme, on a two credit per learning hour basis. A minimum of 12 credits is required in the Patient Outcomes category over a triennium (three years).
Any data driven activity that assesses the outcomes and quality of general practice work can be used to gain credits in the Patient Outcomes learning category. Under the refreshed Te Whanake CPD programme, audits are not compulsory and the RNZCGP also no longer requires that clinical audits are approved prior to use. The college recommends the PDSA format for developing and checking the relevance of a clinical audit.
To claim points go to the RNZCGP website: www.rnzcgp.org.nz
If a clinical audit is completed as part of Te Whanake requirements, the RNZCGP continues to encourage that evidence of participation in the audit be attached to your recorded activity. Evidence can include:
- A summary of the data collected
- An Audit of Medical Practice (CQI) Activity summary sheet (Appendix 1 in this audit or available on the
RNZCGP website).
N.B. Audits can also be completed by other health professionals working in primary care (particularly prescribers), if relevant. Check with your accrediting authority as to documentation requirements.





