Published: August, 2023 | Review date: August, 2026
Recommendations for the treatment of heart failure have changed over time due to the availability of new classes of medicines such as
angiotensin receptor-neprilysin inhibitors (ARNIs) and other treatments, e.g. sodium-glucose co-transporter 2 (SGLT-2) inhibitors.
This audit helps primary healthcare professionals ensure patients diagnosed with heart failure are receiving optimal care.
Heart failure is a complex clinical syndrome that involves abnormalities in the structure or function of the heart, thereby reducing cardiac output and impairing delivery of blood to metabolising tissues. In classical presentations seen in primary care, patients may exhibit features such as ankle swelling, shortness of breath and orthopnoea. However, symptoms and signs can vary substantially depending on the underlying pathology and compensatory mechanisms, and in some cases may only be mild and non-specific, e.g. a reduced exercise capacity and malaise. As a result, recognising heart failure in primary care often relies on the clinician determining whether the combination of symptoms and signs a patient presents with warrant further investigation based on their clinical history. A clinical diagnosis of heart failure can be made if patients are not “ruled-out” based on results of brain natriuretic peptide (BNP) testing; they should also be referred for an echocardiogram to help inform long-term treatment decisions, however, this is not required to make an initial diagnosis.
For further information on identifying and diagnosing patients with heart failure in primary care, see: bpac.org.nz/2022/heart-failure-part-1.aspx
Once heart failure has been diagnosed, pharmacological treatment needs to be initiated as soon as practically possible to improve patient outcomes. The New York Heart Association (NYHA) or World Health Organization (WHO) functional classification systems can help in assessing baseline symptom severity and to guide treatment decisions. Patients are categorised into one of four groups (I – IV) depending on the amount of exertion needed to exacerbate symptoms. The treatment objective is for patients to have no undue fatigue, rapid/irregular heartbeat or breathlessness with mild or ordinary physical activity.
Given that most clinical trial evidence regarding effective management relates to patients with HFrEF, it is practical to initiate treatment in primary care assuming they have this subtype, and then refine management once echocardiology findings become available, if needed. In New Zealand primary care, the conventional approach for pharmacological management in patients with HFrEF has been:
- Immediately prescribe a loop diuretic if the patient has fluid overload
- Initiate an ACE inhibitor or an ARB, and a beta blocker, as soon as possible. These medicines should be started at a low dose and then up-titrated to the maximum tolerated or specified dose (see “Addressing heart failure in primary care: Part 2 - Initiating and escalating treatment for heart failure” or NZF for dosing recommendations).
- If the patient is still symptomatic despite maximum tolerated doses, escalate treatment by adding:
- A mineralocorticoid receptor antagonist (MRA) such as spironolactone (N.B. patients with severe symptoms at presentation can potentially be cautiously initiated on an ACE inhibitor/ARB, beta blocker and spironolactone at the same time according to clinical judgement); and/or
- An ARNI (sacubitril + valsartan) and stop the ACE inhibitor/ARB
- Add additional medicines based on the patient’s co-morbidities, e.g. digoxin, anticoagulants, iron, SGLT-2 inhibitors (discuss self-funding if patients do not qualify for funded treatment, i.e. they do not have diabetes or do not meet the Special Authority criteria)
For further information on initiating and escalating treatment for patients with heart failure in primary care, see: bpac.org.nz/2022/heart-failure-part-2.aspx
The four pillars of heart failure treatment. International guidelines are increasingly recommending that most patients with heart failure should be established on the “four pillars of heart failure treatment” as early as possible, including an ARNI, beta blocker, MRA and SGLT-2 inhibitor (Figure 1A).1, 2 The practical capacity to achieve this combination of medicines will depend on patient co-morbidities and funding restrictions, but should be encouraged where possible to decrease mortality and hospitalisation (Figure 1B),3 and potentially support cardiac structure recovery. Treatment can be initiated and optimised based on a clinical diagnosis of heart failure in primary care (i.e. there is no need to wait for echocardiography); the approach to management can be refined later, if required, once echocardiogram results are available.
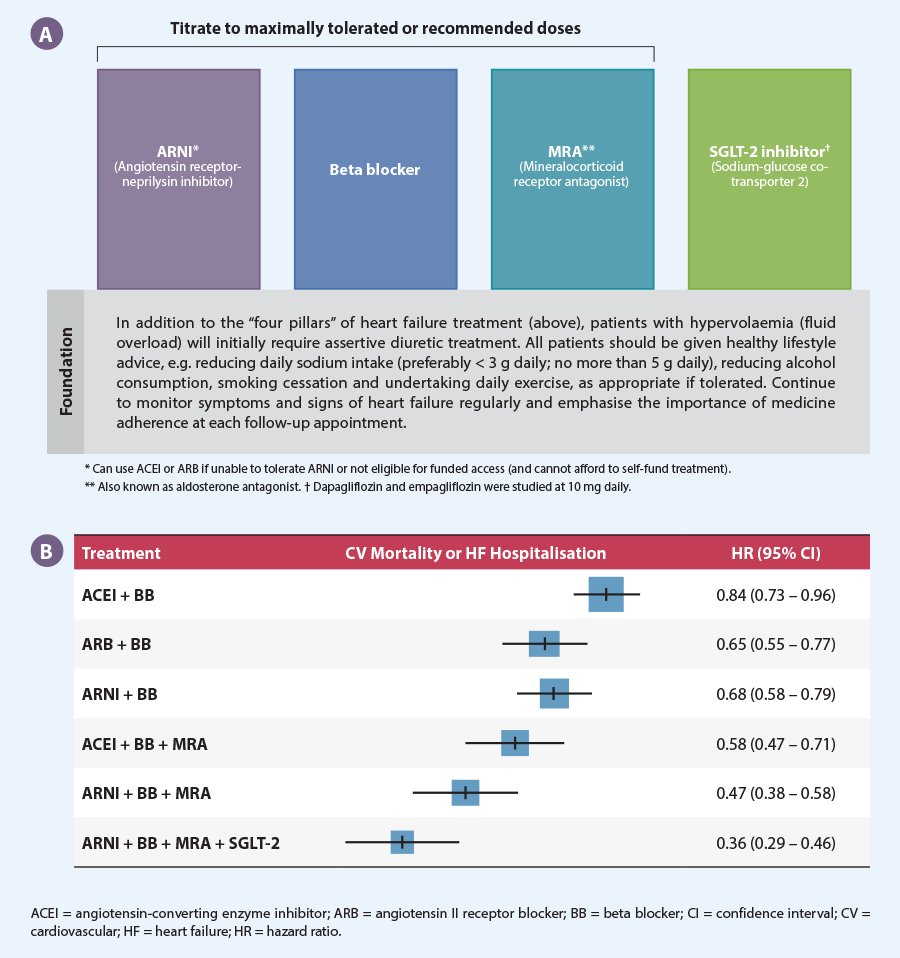
Figure 1. (A) The four pillars of heart failure treatment.1, 2 (B) The risk of cardiovascular mortality or hospitalisation related to heart failure in patients with HFrEF compared with ACE inhibitor treatment alone. Adapted from Tromp et al, 2022.3
A focus on ARNIs
ARNIs are a new class of medicine for treating heart failure, combining an ARB and a neprilysin inhibitor, delivering a dual mechanism of action (Figure 2). Sacubitril + valsartan (Entresto) is the only ARNI currently available. ARNIs were first validated in the PARADIGM-HF trial, where sacubitril + valsartan reduced the absolute risk of cardiovascular death or hospitalisation by almost 5% compared with enalapril in patients with symptomatic heart failure also taking a beta blocker.4 The trial was stopped early after 27 months due to the benefit associated with ARNI use; the NNT was 21 to prevent one primary event involving a composite of CV death or hospitalisation relating to heart failure.4 Subsequent investigation has continued to demonstrate ARNI benefits, including reversal of cardiac remodelling and improved cardiac structure/function,5, 6 as well as significantly enhancing quality of life which is a key treatment objective in patients with heart failure.7
With mounting evidence supporting the use of ARNIs in patients with heart failure, they are now being included as a cornerstone of treatment in recent guidelines. For example, the 2022 AHA/ACC/HFSA Heart Failure guideline states that ACE inhibitors, ARBs and ARNIs are all considered to be first-line options, and that “if patients have chronic symptomatic HFrEF with NYHA class II or III symptoms and they tolerate an ACEi or ARB, they should be switched to an ARNi because of improvement in morbidity and mortality”. While the 2018 National Heart Foundation of Australia (NHFA) and Cardiac Society of Australia and New Zealand (CSANZ) heart failure guidelines are not yet scheduled for a review, a 2022 consensus statement from Australian clinicians also endorses the AHA/ACC/HFSA guideline approach, i.e. prioritising immediate or early ARNI use in patients with HFrEF.
N.B. A 2023 American College of Cardiology consensus decision pathway recommends that ARNIs are also a first-line option for patients with HFpEF (i.e. a documented left ventricular ejection fraction [LVEF] ≥ 50%); however, management decisions are more complex and should usually be made under cardiology guidance, and patients may not meet the current criteria for funded ARNI treatment (see below).
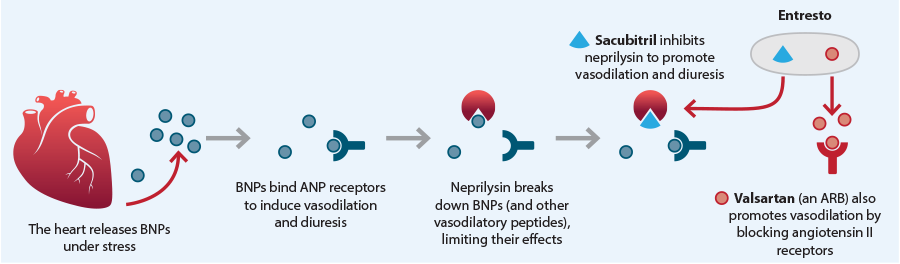
Figure 2. Mechanism of action for the ARNI sacubitril + valsartan (Entresto).
As of August, 2023, Special Authority criteria for funded access to sacubitril with valsartan in New Zealand requires that the patient:
Has heart failure
and
Is in NYHA/WHO functional class II, III or IV
and
Has a documented LVEF ≤ 35%
or
An echocardiogram is not reasonably practical, and in the opinion of the treating practitioner the patient would benefit from treatment
and
Is receiving concomitant optimal standard chronic heart failure treatment
A pragmatic approach to treatment for newly diagnosed patients with heart failure in primary care could be to first initiate them on an ARB (or an ACE inhibitor) and a beta blocker, as soon as possible; if they remain symptomatic despite up-titration, consider whether they would benefit from switching to an ARNI. The timing of this transition will differ depending on individual clinical circumstances, and whether they are already established on these medicines for treating co-morbidities, e.g. hypertension. Initially selecting an ARB, rather than an ACE inhibitor, may be preferable as this more easily facilitates a switch to the ARNI later (ARNIs should not be taken concurrently with an ACE inhibitor or ARB). If transitioning between these treatments, the ARNI can be initiated:
- At least 24 hours after the last dose of ARB, i.e. same time, following day, when the next dose would have been due
- At least 36 hours after the last dose of ACE inhibitor due to the elevated risk of angioedema (see the NZF monograph for further information)
References
- Straw S, McGinlay M, Witte KK. Four pillars of heart failure: contemporary pharmacological therapy for heart failure with reduced ejection fraction. Open Heart 2021;8:e001585. doi:10.1136/openhrt-2021-001585
- Docherty KF, Bayes-Genis A, Butler J, et al. The four pillars of HFrEF therapy: is it time to treat heart failure regardless of ejection fraction? European Heart Journal Supplements 2022;24:L10–9. doi:10.1093/eurheartjsupp/suac113
- Tromp J, Ouwerkerk W, Van Veldhuisen DJ, et al. A systematic review and network meta-analysis of pharmacological treatment of heart failure with reduced ejection fraction. JACC: Heart Failure 2022;10:73–84. doi:10.1016/j.jchf.2021.09.004
- McMurray JJV, Packer M, Desai AS, et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. N Engl J Med 2014;371:993–1004. doi:10.1056/NEJMoa1409077
- Januzzi JL, Prescott MF, Butler J, et al. Association of change in N-terminal pro–B-type natriuretic peptide following initiation of sacubitril-valsartan treatment with cardiac structure and function in patients with heart failure with reduced ejection fraction. JAMA 2019;322:1085. doi:10.1001/jama.2019.12821
- Desai AS, Solomon SD, Shah AM, et al. Effect of sacubitril-valsartan vs enalapril on aortic stiffness in patients with heart failure and reduced ejection fraction: a randomized clinical trial. JAMA 2019;322:1077. doi:10.1001/jama.2019.12843
- Lewis EF, Claggett BL, McMurray JJV, et al. Health-related quality of life outcomes in PARADIGM-HF. Circ: Heart Failure 2017;10:e003430. doi:10.1161/CIRCHEARTFAILURE.116.003430
Summary
This audit identifies patients who have been diagnosed with heart failure for at least three months, and either have HFrEF or an undifferentiated clinical diagnosis, to determine if their treatment regimen remains appropriate or whether they may benefit from taking an ARNI and/or other treatment(s), e.g. spironolactone, SGLT-2 inhibitors. This audit does not focus on patients with confirmed HFpEF as management differs and should ideally be directed by cardiology guidance.
A three-month minimum timeframe was selected for the purposes of this audit to encompass a reasonable treatment initiation and up-titration period, which may differ depending on individual patient characteristics and circumstances. In general, up-titration of ACE inhibitors/ARBs and beta blockers involves doubling doses no sooner than every two to four weeks in primary care, up to the maximum tolerated or recommended maintenance dose. However, clinicians may consider earlier use of other medicines (e.g. spironolactone, SGLT-2 inhibitors) and/or an ARNI, if appropriate (e.g. in accordance with recommendations from the 2022 AHA/ACC/HFSA Heart Failure guideline and Australian clinician consensus statement on heart failure).
Recommended audit standards
At a minimum, all patients with a clinical diagnosis of heart failure should have been initiated on an ACE inhibitor/ARB and a beta blocker unless contraindicated. These medicines should have been up-titrated to the maximum recommended or tolerated dose, and other medicines may have been added to the regimen. There should be documentation in patient notes indicating they remain asymptomatic with ordinary or mild physical activity, e.g. daily tasks such as getting dressed, having a shower, walking around the house.
If these criteria are not met, the patient should be flagged for review to determine the appropriate next step(s), depending on their clinical circumstances. This may include deciding whether:
- Dose increases for current medicines are warranted, e.g. dose has not yet been up-titrated
- The patient should switch to an ARNI (and stop the ACE inhibitor/ARB). For further information on ARNI initiation and monitoring considerations, see: nzf.org.nz/nzf_70779
- A MRA (e.g. spironolactone) or SGLT-2 inhibitor should be introduced
- Cardiology advice or referral is required
Eligible patients
All patients who have been diagnosed with heart failure for at least three months and are identified as having either HFrEF or an undifferentiated clinical diagnosis (i.e. echocardiography has not yet been performed) are eligible for this audit. Patients with HFpEF can be excluded.
Identifying patients
You will need to have a system in place that allows you to identify eligible patients. Many practices will be able to identify patients by running a “query” through their PMS, initially searching for all patients with heart failure. The clinical notes of identified patients will need to be reviewed to ascertain the duration and type (to confirm eligibility) as well as treatment details, including their current regimen and symptom status (to determine audit outcome).
Sample size
The number of eligible patients will vary according to your practice demographic, and for some practices the initial query may return a large number of results. If this occurs, a sample size of 20 – 30 patients is sufficient for this audit (N.B. the principles of this audit should still be considered opportunistically in any consultation involving a patient with heart failure).
Criteria for a positive outcome
A positive outcome is achieved if an eligible patient is currently receiving optimal standard chronic heart failure treatment and at their last clinical review reported being asymptomatic with ordinary or mild physical activity (i.e. NYHA functional class I).
Data analysis
Use the sheet provided to record your data. The percentage achievement can be calculated by dividing the number of patients with a positive outcome by the total number of patients.
Patients who do not meet the criteria for a positive result should be flagged for clinical review to consider how treatment can be optimised (see: “Recommended audit standards”).

This publication was supported by an unrestricted educational grant by Novartis NZ Ltd. The publication was independently written and Novartis had no control over the content. The views expressed in this publication are those of the author and not necessarily those of Novartis
Clinical audits can be an important tool to identify where gaps exist between expected and actual performance. Once completed, they can provide ideas on how to change practice and improve patient outcomes. General practitioners are encouraged to discuss the suitability and relevance of their proposed audit with their practice or peer group prior to commencement to ensure the relevance of the audit. Outcomes of the audit should also be discussed with the practice or peer group; this may be recorded as a learning activity reflection if suitable.
The Plan, Do, Study, Act (PDSA) model is recommended by the Royal New Zealand College of General Practitioners (RNZCGP) as a framework for assessing whether a clinical audit is relevant to your practice. This model has been widely used in healthcare settings since 2000. It consists of two parts, the framework and the PDSA cycle itself, as shown in Figure 3.
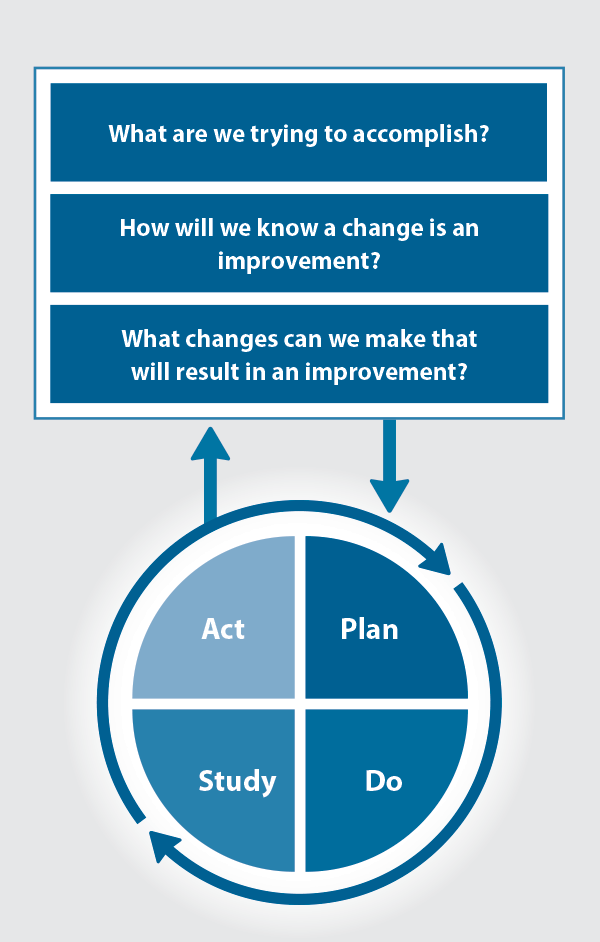
Figure 3. The PDSA model for improvement.
Source: Plan, Do, Study, Act (PDSA) cycles and the model for improvement
1. The framework
This consists of three questions that help define the “what” and “how” of an improvement project (in this case an audit).
The questions are:
- "What are we trying to accomplish?" – the aim
- "How will we know that a change is an improvement?" – what measures of success will be used?
- "What changes can we make that will result in improvement?" – the concept to be tested
2. The PDSA cycle
This is often referred to as the “engine” for creating, testing and carrying out the proposed changes. More than one cycle is usually required; each one is intended to be short, rapid and frequent, with the results used to inform and refine the next. This allows an ongoing process of continuous learning and improvement.
Each PDSA cycle includes four stages:
- Plan – decide what the change to be tested is and how this will be done
- Do – carry out the plan and collect the data
- Study – analyse the data, assess the impact of the change and reflect on what was learned
- Act – plan the next cycle or implement the changes from your plan

Claiming credits for Te Whanake CPD programme requirements
Practice or clinical audits are useful tools for improving clinical practice and credits can be claimed towards the Patient Outcomes (Improving Patient Care and Health Outcomes) learning category of the Te Whanake CPD programme, on a credit per learning hour basis. A minimum of 12 credits is required in the Patient Outcomes category over a triennium (three years).
Any data driven activity that assesses the outcomes and quality of general practice work can be used to gain credits in the Patient Outcomes learning category. Under the refreshed Te Whanake CPD programme, audits are not compulsory and the RNZCGP also no longer requires that clinical audits are approved prior to use. The college recommends the PDSA format for developing and checking the relevance of a clinical audit.
To claim points go to the RNZCGP website: www.rnzcgp.org.nz
If a clinical audit is completed as part of Te Whanake requirements, the RNZCGP continues to encourage that evidence of participation in the audit be attached to your recorded activity. Evidence can include:
- A summary of the data collected
- An Audit of Medical Practice (CQI) Activity summary sheet (Appendix 1 in this audit or available on the
RNZCGP website).
N.B. Audits can also be completed by other health professionals working in primary care (particularly prescribers), if relevant. Check with your accrediting authority as to documentation requirements.





