Ingrown toenails primarily affect younger males
Ingrown toenails, also known as onychocryptosis or unguis incarnates, are a painful condition due to the sides or corner
of the toenail digging into the surrounding soft tissue. This results in a breach of the underlying skin and leads to
pain, inflammation, formation of granulation tissue, and in some cases infection. The most commonly affected area is the
lateral edge of the great (big) toe, although the medial edge and other toes can also be affected. Ingrown toenails most
frequently occur in males aged 15–40 years.1 It has been reported that approximately 20% of patients who present to their
general practitioner with foot problems will have an ingrown toenail.2
The exact causes of ingrown toenails are still being debated
A number of intrinsic and extrinsic factors have traditionally been linked with the development of ingrown
toenails. However, there is a lack of quality evidence supporting a single mechanism and ingrown toenail development
may be triggered by multiple factors. There is ongoing debate about whether factors relating to the nail itself
are responsible for the condition or whether the size and shape of the surrounding periungual nail folds are
the cause (Figure 1).3
Factors traditionally associated with the development of ingrown toenails, and supported by varying degrees of evidence,
include:2, 4
- Inappropriate nail trimming which can cause the corner of the nail to dig in to the surrounding skin (see: “Toenail
cutting - advice for patients”)
- Tight or narrow footwear which can compress the toes and result in changes in the shape of the toenail
- Hyperhidrosis and poor foot hygiene
- Onychomycosis (fungal nail infection)
- A family history of ingrown toenails
- Repetitive trauma, e.g. running, kicking or stubbing of the toe
- Abnormally shaped nail plates or nail folds
- Diabetes and obesity
- Thyroid, cardiac and renal disorders
- Some medicines, e.g. retinoids, oral antifungals, ciclosporin and docetaxel (an IV chemotherapy medicine)
Treatment of ingrown toenails includes non-surgical and surgical options
Patients with an ingrown toenail most frequently present with pain, redness and swelling, the severity of which depends
on the stage of the ingrown toenail (Table 1) and whether any infection is present. Although clinical staging of an ingrown
toenail is not always necessary, being aware of the different stages can help in selecting the most appropriate treatment.
Diagnostic tests are not usually required, but if a particular cause is suspected appropriate tests can be ordered,
e.g. nail clippings and scrapings of subungual debris for fungal culture and microscopy.
When deciding on the most appropriate treatment method to manage a patient with an ingrown toenail a number of factors
need to be taken into consideration, including:
- The severity of the pain and inflammation and if infection is present
- Whether the patient has previously presented with an ingrown toenail
- What treatments have been previously tried and if the treatment was successful
- Patient preference and co-morbidities, e.g. some people may not like the cosmetic results of surgical options and
people with certain co-morbidities, e.g. diabetes, may not be candidates for some surgical treatments
In general, conservative treatments can be trialled in patients with a first presentation of an ingrown toenail with
mild symptoms, in those who do not want to have surgery and in those at an increased risk of surgical complications. Patients
with more severe symptoms or with an ingrown toenail that has not responded to conservative treatment can be considered
for surgical options.
A 2012 Cochrane review reported that surgical interventions are generally more effective in preventing recurrence of
an ingrown toenail than non-surgical treatments.5 However, the review did not define which stages of ingrown toenails
were included in the trials and the results are likely to be more applicable for patients with a moderate-to-severe ingrown
toenail.
Conservative options can be tried in patients with mild ingrown toenails
There are a number of general measures and conservative treatments that can be considered in patients with a mild ingrown
toenail.
General measures: May not “cure” the ingrown toenail, but can provide symptomatic relief and prevent
the ingrown toenail from becoming infected or progressing to the next stage. The following can be considered:4
- Gently lifting the nail and removing the spicule (small spike at outer margin of nail plate) that is digging in to
the surrounding soft tissue (if the patient has not already tried this or has not performed the procedure effectively)
- Treating any underlying pathogenic factors, e.g. confirmed fungal infection, hyperhidrosis
- Applying silver nitrate to cauterise the granulation tissue and reduce the skin fold bulk. This can, however, be a
slow process and it may be more effective to remove the granulation tissue later if surgery is undertaken.
- Cleaning the area with hydrogen peroxide or iodine solution to slow or stop the growth of micro-organisms
- Instructing the patient to gently massage the inflamed area at night
- Educating the patient about wearing appropriate footwear that fits well and does not result in excessive bunching
of the toes, e.g. wearing shoes with a wide toe box or open toe
People with a fungal toenail infection have an increased risk of developing an ingrown toenail as the fungal infection
causes the toenail to become thickened. Patients often require treatment with an oral antifungal, e.g. terbinafine or
itraconazole, or a topical antifungal, e.g. amorolfine or ciclopirox, in combination with the ingrown toenail treatment.
 For further information, see “Management
of fungal nail infections” BPJ 19 (Feb, 2009).
For further information, see “Management
of fungal nail infections” BPJ 19 (Feb, 2009).
Antibiotics: The use of antibiotics in patients with an ingrown toenail appears to be primarily based
on historical practice and there is limited clinical trial evidence supporting their routine use.2, 7 Antibiotics
may be considered when a patient presents with obvious signs of infection, e.g. erythema, pus and some evidence of extending
cellulitis, especially if the infection extends beyond the nail fold. However, it can be difficult to differentiate between
infection and non-infective inflammation. If it is decided that antibiotics are warranted, the antibiotic selected should
have cover against Staphylococcus aureus, e.g. flucloxacillin, as this is the bacteria most commonly associated with nail
fold infections.2
Antibiotics have also traditionally been prescribed to reduce any infection prior to surgery. However, it has been reported
that once the ingrown part of the toenail has been surgically removed and chemical matricectomy with phenol performed,
the localised infection/inflammation resolves without the need for antibiotics.2 Antibiotics are also not
routinely required when the surgical treatment targets the surrounding skin folds.8
Toenail cutting – advice for patients
Inappropriate toenail trimming is associated with the formation of ingrown toenails and conventional advice to prevent
this is for toenails to be cut straight across rather than curved.5 However, this advice has been challenged more recently.
A study that investigated two different surgical techniques in patients with an ingrown toenail reported that the toenail
cutting method (straight vs. curved) was not a significant factor in ingrown toenail development.6 The overall shape of
the nail is determined by the growing area at the nail matrix.
Patients can be advised to:
- Cut their toenails either straight across or with a gentle curve, taking care not to cut too deeply down into the
corners of the nail; podiatry grade clippers may be required to cut tough, thick nails
- Use a nail file to prevent jagged edges and create a smooth, rounded edge. A Black’s file (a thin file designed to
clear debris from the nail sulcus [gutter] and file the edge of the nail) can be recommended as the thin design helps
to access difficult to reach areas, e.g. the spicule
Patients with mobility or flexibility problems or very thickened nails may need to be referred to a podiatrist for nail
cutting.
Non-surgical treatment strategies
There are a number of non-surgical options available that target either the ingrown toenail itself or the surrounding
nail folds. The aim of conservative treatment is to separate the ingrown part of the toenail from the surrounding nail
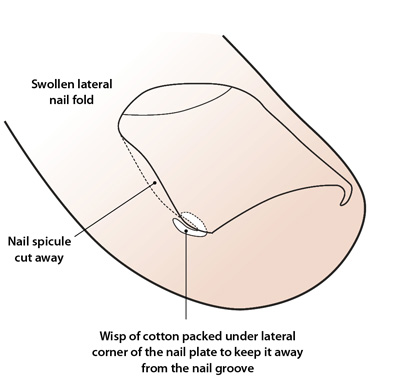
fold. The cotton wick method is the most commonly performed of these methods in general practice.
The cotton wick (packing) method: Involves elevating the lateral edge of the toenail and inserting
a small piece of cotton wick (which can be soaked in disinfectant or antiseptic) under the edge of the nail to prevent
it digging in to the surrounding tissue (Figure 2).4 The procedure can generally be performed
without the use of a local anaesthetic. If necessary, silver nitrate can be used to cauterise any surrounding granulation
tissue. Be aware that silver nitrate is corrosive and stains both the toenail and surrounding tissue black. Patients usually
report immediate relief of pain after the procedure. The patient can be instructed to repeat the process once, or if necessary,
twice daily, or if the cotton falls out. It is generally recommended that the cotton wick only remain in place for approximately
one week as distal subungual onychomycosis can develop if the cotton wick is left in for a prolonged period.
Dental floss technique: This technique is similar to the cotton wick method except that a string of
dental floss is used to separate the toenail and the nail bed rather than a cotton wick. The dental floss is inserted
obliquely under the corner of the ingrown toenail and pushed proximally. The procedure is usually performed without a
local anaesthetic. It has been reported that patients experience immediate relief of pain, followed by growing out of
the spicule without injury to the nail fold.9 The dental floss is usually left in place until the lateral
anterior tip of the of the nail plate reaches the hyponychium (Figure 1).9 The dental
floss should be replaced if it becomes dirty or falls out before this occurs.
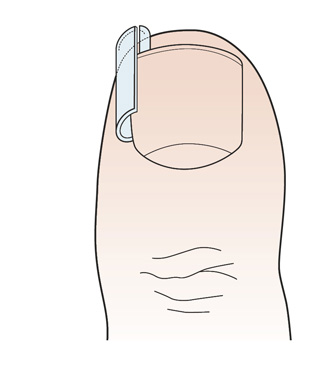
The gutter splint (sleeve) technique: A small sterile plastic tube, most commonly from an IV line,
is split lengthways (with a diagonal cut on one end to aid smooth insertion) and inserted under the lateral edge of the
nail (Figure 3). The nail corner and lateral edge of the nail is lifted and the “gutter” slid down
so that it rests between the nail and the underlying soft tissue. A local anaesthetic is required when performing the
procedure.10 The gutter can be fixed in place with adhesive tape, sutures or an acrylic resin. The gutter
splint can then be covered with an appropriate dressing to stop it catching on clothing and bed sheets. The length of
time the gutter is left in place depends on the time required for the normal nail to grow over the tip of the toe and
can range from two weeks to three months.2 The technique has been reported to be highly effective – one study
reported no recurrences in 62 patients who underwent the procedure.10
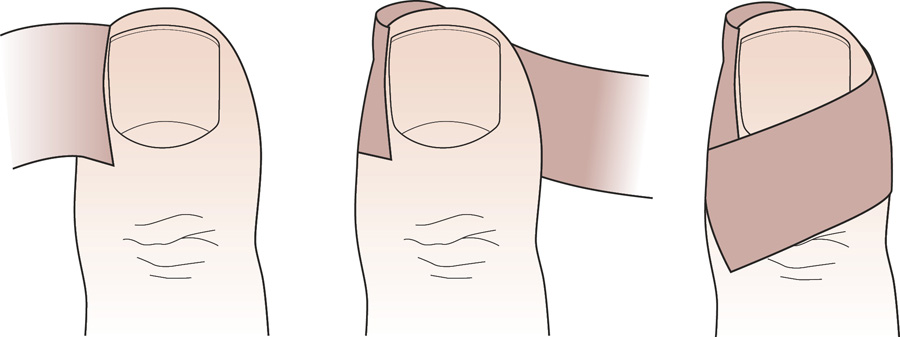
Taping method: This technique is the least invasive of all the conservative non-surgical treatments
and uses an adhesive elastic tape, e.g. strapping tape (approximately 15 – 20 mm wide and 5 cm long), to pull the lateral
nail fold away from the ingrown toenail (Figure 4).7 One end of the elastic tape is placed
against the ingrown nail alongside any granulation tissue (if present) and then wrapped around the toe so that the other
end overlaps the first without covering the toenail.11 The exact taping technique is crucial and patients
will require specific instruction about how to perform it.7 It is generally recommended that the affected
toe is re-taped every three to seven days (or when the tape becomes ineffective) for at least two months.
Orthoyxia (brace technique): This technique uses a small metal brace to pull the edge of the ingrown
toenail away from the underlying soft tissue, after removal of the spicule. However, these braces are not readily available
in New Zealand. A study that investigated nail bracing in patients with an ingrown toenail reported that all 12 patients
were pain-free after six to 10 months of treatment.13
Angle correction technique: This technique aims to correct the convex nature of the toenail by filing
the entire surface of it with the intention of decreasing its thickness by 50–75%. The process is then repeated by the
patient every two months making the nail thin and soft which reduces the pressure on the nail fold. A Blacks file (a specialised
nail file – see “Toenail cutting”) can then be used to reshape the edge of the nail. Patients
need to be educated about the importance of not removing too much of the toenail as this can result in pain when pressure
is placed on the nail.
 |
 |
| Figure 2: The cotton wick (packing) method |
Figure 3: The gutter splint (sleeve) technique |
 |
| Figure 4: The taping method |
Surgical treatment options: techniques target either the nail or the soft tissue
Most surgical techniques for correcting an ingrown toenail are variations of two different approaches which either target
the nail plate itself or the lateral skin folds that surround the toenail. Surgical treatments have traditionally focused
on the nail as the causative agent, and the most commonly performed procedure is the “wedge resection” technique that
involves partial removal of the toenail with segmental phenol ablation.5
Recent evidence suggests that a surgical technique that targets the nail folds and leaves the toenail intact (based
on the “Vandenbos” technique) should be considered more often, as very low recurrence rates have
been reported.8
Surgical treatments that target the toenail
There are a number of different techniques that target the toenail. Most are variations of the widely used “wedge resection”
technique which involves removal of the affected margin of the ingrown toenail. After avulsion of the affected portion
of the toenail, destruction of the nail matrix prevents that part of the nail re-growing (therefore permanently reducing
the width of the toenail). There are a number of methods used for destruction of the nail matrix including liquefied phenol
(90%), sodium hydroxide (10 – 20%), surgical dissection, diathermy, electrocautery and carbon dioxide laser. Of these,
phenol is the most commonly used and has been shown to be effective in preventing recurrence.5
Partial nail avulsion (wedge resection) with segmental phenol ablation
This procedure is performed under a partial ring block with 1% plain lidocaine injected at the base of the toe. As the
major innervations to the nail plate are the plantar digital proper nerves, the majority of the local anaesthetic should
be placed on the plantar aspect of the digit. A three-sided ring block is recommended as a four-sided block is associated
with a risk of ischaemia.14 A ring tourniquet is applied to the toe followed by longitudinal removal of the
outer part (usually 3 – 5 mm) of the affected toenail, including the nail matrix. Segmental ablation of the exposed toenail
matrix is then performed using liquefied phenol. There is some debate about the length of time that the phenol should
be applied for, but two 60-second applications appears to be most widely used.1 Other studies have reported
that phenol only needs to be applied for 60 seconds in total, which can be split into three 20 second applications.15 The
applications should be separated by a washout with saline (alcohol is often used but is unnecessary) and this should be
repeated after each application of phenol.1 The area should be dried with a cotton wool swab prior to each
application of the phenol to reduce the chance that the phenol will be diluted with blood or saline.
Postoperative care: The patient should be advised to keep their leg elevated for 24 – 48 hours while
seated and avoid wearing a shoe on the affected foot for approximately three days. Antibiotics are not routinely required
as it has been reported that postoperative antibiotic prophylaxis does not reduce the rate of postoperative infection
or recurrence of the ingrown toenail.5, 6 The patient can remove the dressing on the day after surgery and
soak the affected foot in warm water containing Epsom salts, twice daily, for approximately one week. Table salt
(one to three tablespoons per litre of water) can be used as an alternative to Epsom salts. Patients may require analgesia,
e.g. paracetamol +/- codeine or ibuprofen, for two to three days. Follow-up check of the site at one week is
recommended (Figure 5).
The recurrence rates following this procedure vary from 1 – 14%.6, 7 A 2006 randomised study that compared
partial nail avulsion with or without phenol ablation of the matrix reported that the one-year recurrence rates were significantly
lower when phenol ablation was used (14% vs. 41%).6
This technique can be performed in patients with diabetes as it is not contraindicated in the presence of an impaired
arterial blood supply.7 The procedure can also be used safely in children (although it is rarely performed),
usually after conservative treatments have failed.7
Longitudinal band method
This technique involves longitudinal removal of the middle 4 – 5 mm of the affected toenail as far back as the skin
at the base of the toenail, i.e. the most distal portion of the nail and nail matrix are left intact. Although limited
clinical trial data are available for this technique, the advantages appear to include low recurrence rates (approximately
2%) and minimal limitation of daily functioning.16
Total nail avulsion not recommended
Total removal of the nail without phenol ablation is not recommended because overall recurrence rates of approximately
70% have been reported in a number of studies.8 Total removal of the nail with matricectomy is generally considered
to be an obsolete technique.7
Surgical treatments that target the lateral nail fold
Surgical techniques that target the lateral periungal soft tissue nail fold were first described by Vandenbos and Bowers
in the late 1950s.17 Recent research suggests that the “Vandenbos” technique results in very low or “zero”
recurrence rates (see below) and provides an alternative surgical option for ingrown toenails.8, 18
Excision of the nail fold (based on the Vandenbos technique)
This procedure involves extensive removal of the periungal nail fold while leaving the toenail itself intact. The procedure
is performed under a three-sided ring block of the affected toe and involves making a large elliptical incision on each
side of the nail and removing the relevant lateral skin folds. It is important that the excision is generous and adequate
(leaving a soft tissue deficiency of approximately 1.5 × 3 cm). Light cauterisation with either silver nitrate or electrocautery
is then performed and the wound is left to heal by secondary intention.8 A gauze dressing should be applied.
Postoperative care: The patient should be instructed to remove the gauze dressing after 48 hours and
to soak their feet in a warm water bath containing Epsom salts for 15 – 20 minutes.18 Table salt (one to three
tablespoons per litre of water) can be used as an alternative to Epsom salts. A new dressing can then be reapplied and
the procedure repeated up to three times a day for the next four to six weeks, although patients are often not adherent
with this.8 Paracetamol +/- codeine or ibuprofen are usually sufficient for pain relief in the immediate postoperative
period. Antibiotics are not routinely required.18 Ideally, the patient should be followed-up after two weeks.
The wound should be healed after four to six weeks with the nail sitting above the surrounding soft tissue.18
Two studies that examined the Vandenbos-based technique reported no recurrences of ingrown toenails after the procedure,
no cases of osteomyelitis, and high rates of patient satisfaction due to good cosmetic results.8, 18
N.B. The Vandenbos technique is not recommended in patients with diabetes as poor blood supply can delay healing. Partial
nail avulsion with phenol ablation is recommended in these patients.
 Instructional videos for many of the surgical procedures for treating ingrown
toenails can be found on YouTube.
Instructional videos for many of the surgical procedures for treating ingrown
toenails can be found on YouTube.
Acknowledgement
Thank you to Dr Daniel Poratt, Podiatric Surgeon, Senior Lecturer in Podiatry, Auckland University of Technology and
Dr Amanda Oakley, Specialist Dermatologist, Clinical Associate Professor, Tristram Clinic, Hamilton for expert review of this article.