In this report 
View
/ Download pdf version of this report
New Zealand has one of the highest rates of childhood asthma in the world.1 It is the leading cause of
sleep disturbance, missed school days and hospital admissions in children, and more than one in four children have some
form of asthma or asthma symptoms.2 Asthma affects Māori and Pacific children disproportionately to other
children in New Zealand.
This report highlights some of the messages featured in “Diagnosing and
managing asthma in children” from Best Practice Journal 42, February 2012.
The report covers the first three steps of the stepwise treatment guidelines in the BPJ article and shows the proportion
of patients on each step by ethnicity to highlight some of the ethnic disparaties in asthma treatment that are observed
in New Zealand.
Additional management beyond Step Three focuses on increasing treatment with inhaled corticosteroids (ICS), or the addition
of oral steroids, and referral to a paediatrician.
In this report, a patient is defined as a child aged under 15 years who was dispensed two or more short-acting beta-2
agonists (SABA) inhalers between 1 November 2010 and 31 October 2011.
Treatment Steps
| Step One |
Mild, intermittent asthma – SABA alone
Children with symptomatic asthma should be prescribed short-acting beta-2 agonists (SABA) such as salbutamol or terbutaline.
Māori and Pacific children have a greater frequency of severe asthma3 than children of other ethnic
groups, and may benefit from more intensive initial treatment than Step One. |
| Step Two |
More severe asthma, or symptoms uncontrolled – SABA and ICS
The addition of inhaled corticosteroids (ICS) may be beneficial for children whose symptoms are uncontrolled on Step
One or whose asthma symptoms are more severe. |
| Step Three |
Control not achieved at Step Two – add LABA
If control is not achieved with a SABA and an ICS preventer then additional treatment will be needed. For children
aged 5 – 12 years a long acting beta agonist (LABA) should be considered. |
National data by ethnicity
The chart below shows the proportion of patients in New Zealand, dispensed medicines relating to each asthma management
step, by ethnicity.
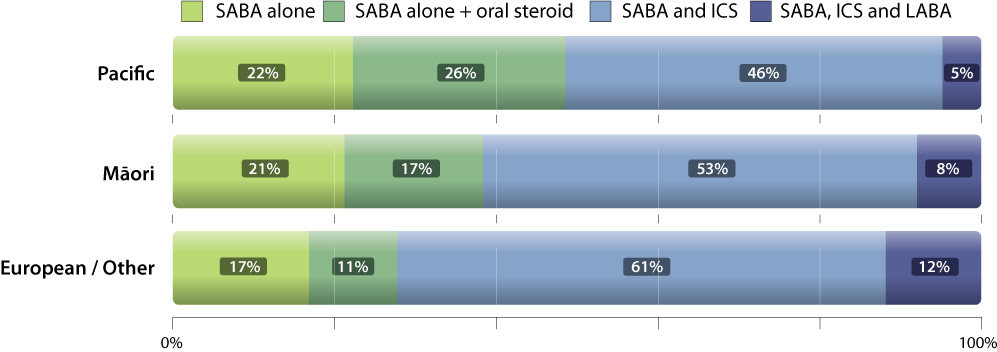
Although a greater proportion of Māori and Pacific children are on Step One - SABA alone, these children appear
to be less well controlled at this step; a larger proportion of Māori and Pacific children (p < 0.01) were dispensed
an oral steroid at least once compared with European/other children.
A larger proportion of European/other children are on Step Two - SABA and ICS compared to Māori and Pacific children.
Māori and Pacific children are also less likely to have their treatment escalated to Step Three - SABA, ICS and
LABA (p < 0.01) than European/other children. This is despite the fact that Māori and Pacific children are known
to have a greater prevalence and severity of asthma symptoms.
 Practice/peer group debate: The data in this report is based
on medicines dispensed. Do the ethnic disparities highlighted in the report suggest that there are difficulties in accessing
medicines for Māori and Pacific peoples or is asthma prescribing in New Zealand influenced by ethnicity?
Practice/peer group debate: The data in this report is based
on medicines dispensed. Do the ethnic disparities highlighted in the report suggest that there are difficulties in accessing
medicines for Māori and Pacific peoples or is asthma prescribing in New Zealand influenced by ethnicity?
Notes
- The data in this report includes dispensings recorded in the New Zealand Health Information Services data collections
for all SABA, ICS, LABA and Oral Steroids dispensed to children under 15 between 1 November 2010 and 31 October 2011.
- The significance tests used are Yates’s χ2 tests.
- Some numbers may be affected by rounding.
Further reading
References
- Asher MI, Stewart A, Clayton T, et al. Has the prevalence and severity of symptoms of asthma changed among children
in New Zealand? ISAAC Phase Three. N Z Med J 2008;212(1284).
- ISSAC. The Global Asthma Report. Paris, France: The international union against tuberculosis and lung disease, 2011.
- Pattermore P, Ellison-Loschmann L, Asher MI, et al. Asthma prevalence in European, Māori and Pacific children
in New Zealand: ISAAC study. Pediatr Pulmonol 2004;37(5):433-42.